

Continuity of care with physicians and risk of subsequent hospitalization and end-stage renal disease in newly diagnosed type 2 diabetes mellitus patients
- PMID: 29559787
- PMCID: PMC5856058
- DOI: 10.2147/TCRM.S150638
Continuity of care with physicians and risk of subsequent hospitalization and end-stage renal disease in newly diagnosed type 2 diabetes mellitus patients
Abstract
Purpose: Effective management for type 2 diabetes mellitus (DM) can slow the progression of kidney outcomes and reduce hospital admissions. Better continuity of care (COC) was found to improve patients' adherence and self-management. This study examined the associations between COC, hospitalization, and end-stage renal disease (ESRD) in DM patients.
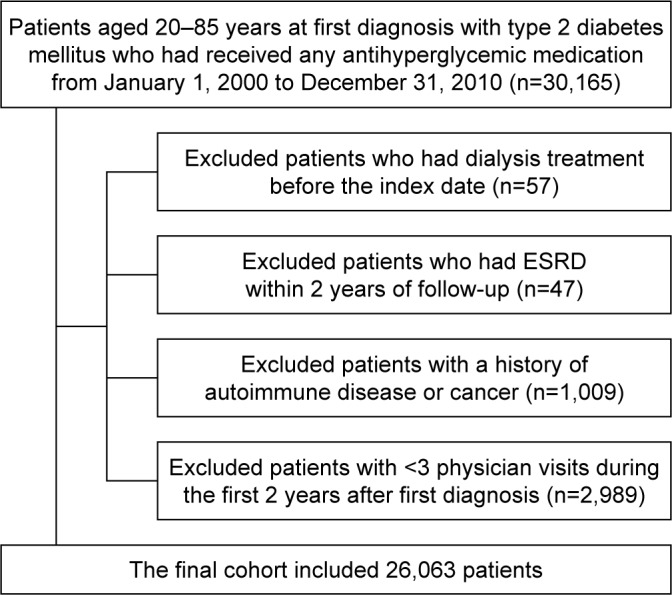
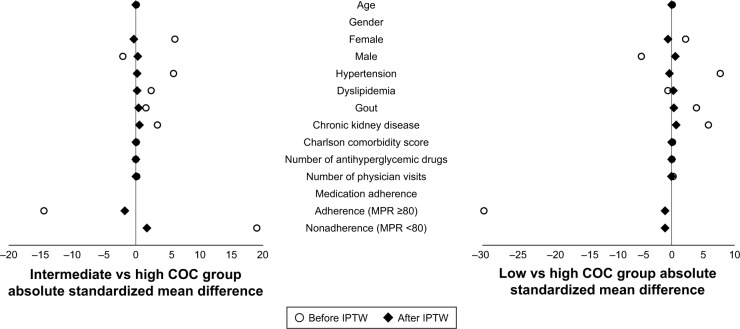
Patients and methods: In the cohort study, data from 1996 to 2012 were retrieved from the Longitudinal Health Insurance Database, using inverse probability weighted analysis. A total of 26,063 patients with newly diagnosed type 2 DM who had been treated with antihyperglycemic agents were included. COC is to assess the extent to which a DM patient visited the same physician during the study period. This study categorized COC into 3 groups - low, intermediate, and high, - according to the distribution of scores in our sample.
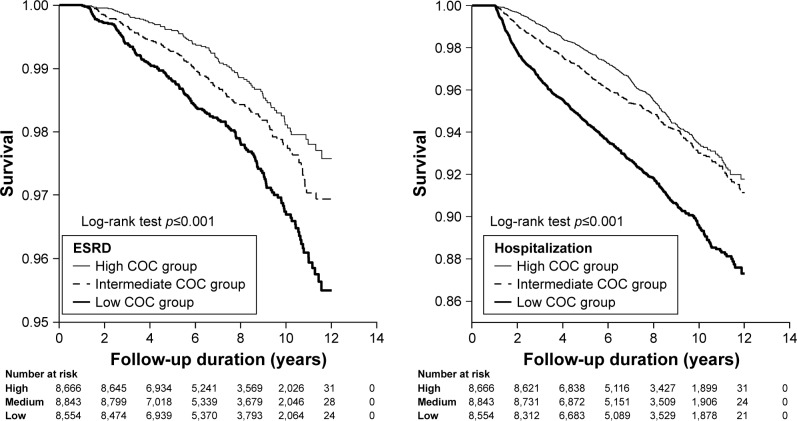
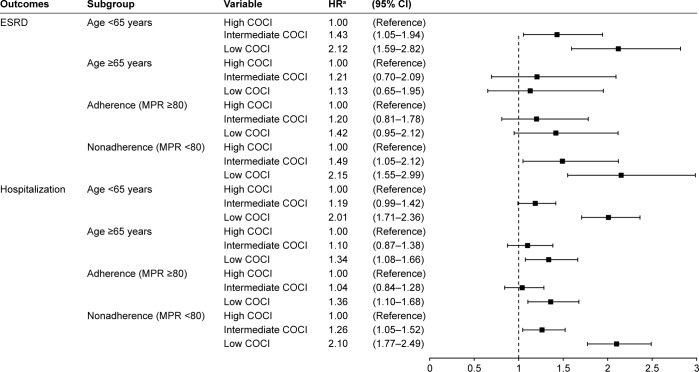
Results: The number of ESRD patients in the high, intermediate, and low COC groups were 92 (22.33%), 130 (31.55%), and 190 (46.12%), respectively, and the mean follow-up periods for the 3 groups were 7.13, 7.12, and 7.27 years, respectively. After using inverse probability weighting, the intermediate and low COC groups were significantly associated with an increased risk of ESRD compared with the high COC group (adjusted hazard ratio (aHR) 1.36 [95% CI, 1.03-1.80] and aHR 1.76 [95% CI, 1.35-2.30], respectively). The intermediate and low COC groups were also significantly associated with the subsequent hospitalization compared with the high COC group (aHR 1.15 [95% CI, 0.99-1.33] and aHR 1.72 [95% CI, 1.50-1.97], respectively).
Conclusion: COC is related to ESRD onset and subsequent hospitalization among patients with DM. This study suggested that when DM patients keep visiting the same physician for managing their diseases, the progression of renal disease can be prevented.
Keywords: continuity of care; diabetes mellitus; end-stage renal disease; hospitalization.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Effects of continuity of care on the postradiotherapy survival of working-age patients with oral cavity cancer: A nationwide population-based cohort study in Taiwan.PLoS One. 2019 Dec 16;14(12):e0225635. doi: 10.1371/journal.pone.0225635. eCollection 2019. PLoS One. 2019. PMID: 31841525 Free PMC article.
-
The effect of continuity of care on the incidence of end-stage renal disease in patients with newly detected type 2 diabetic nephropathy: a retrospective cohort study.BMC Nephrol. 2018 Jun 5;19(1):127. doi: 10.1186/s12882-018-0932-3. BMC Nephrol. 2018. PMID: 29871604 Free PMC article.
-
Impact of potentially inappropriate medication and continuity of care in a sample of Taiwan elderly patients with diabetes mellitus who have also experienced heart failure.Geriatr Gerontol Int. 2016 Oct;16(10):1117-1126. doi: 10.1111/ggi.12606. Epub 2015 Oct 23. Geriatr Gerontol Int. 2016. PMID: 26492893
-
Losartan and other angiotensin II antagonists for nephropathy in type 2 diabetes mellitus: a review of the clinical trial evidence.Clin Ther. 2003 Dec;25(12):3044-64. doi: 10.1016/s0149-2918(03)90091-9. Clin Ther. 2003. PMID: 14749145 Review.
-
Continuity of outpatient care and avoidable hospitalization: a systematic review.Am J Manag Care. 2019 Apr 1;25(4):e126-e134. Am J Manag Care. 2019. PMID: 30986022
Cited by
-
Qualitative study of pathways to care among adults with diabetes in rural Guatemala.BMJ Open. 2023 Jan 6;13(1):e056913. doi: 10.1136/bmjopen-2021-056913. BMJ Open. 2023. PMID: 36609334 Free PMC article.
-
Effects of continuity of care on the postradiotherapy survival of working-age patients with oral cavity cancer: A nationwide population-based cohort study in Taiwan.PLoS One. 2019 Dec 16;14(12):e0225635. doi: 10.1371/journal.pone.0225635. eCollection 2019. PLoS One. 2019. PMID: 31841525 Free PMC article.
-
Effects of continuity of care on health outcomes among patients with diabetes mellitus and/or hypertension: a systematic review.BMC Fam Pract. 2021 Jul 3;22(1):145. doi: 10.1186/s12875-021-01493-x. BMC Fam Pract. 2021. PMID: 34217212 Free PMC article.
-
Glycemic Control, Renal Progression, and Use of Telemedicine Phone Consultations Among Japanese Patients With Type 2 Diabetes Mellitus During the COVID-19 Pandemic: Retrospective Cohort Study.JMIR Diabetes. 2023 Nov 21;8:e42607. doi: 10.2196/42607. JMIR Diabetes. 2023. PMID: 37315193 Free PMC article.
-
Exploring health literacy in patients with chronic kidney disease: a qualitative study.BMC Nephrol. 2020 Jul 29;21(1):314. doi: 10.1186/s12882-020-01973-9. BMC Nephrol. 2020. PMID: 32727397 Free PMC article.
References
-
- World Health Organization Global Report on Diabetes. 2016. [Accessed February 26, 2018]. Available from: http://apps.who.int/iris/bitstream/10665/204871/1/9789241565257_eng.pdf.
-
- Shen FC, Chen CY, Su SC, Liu RT. The prevalence and risk factors of diabetic nephropathy in Taiwanese type 2 diabetes – a hospital based study. Acta Nephrologica. 2009;23:90–95.
LinkOut - more resources
Full Text Sources
Other Literature Sources
