

Is pharmacologic treatment better than neural mobilization for cervicobrachial pain? A randomized clinical trial
- PMID: 29559834
- PMCID: PMC5859768
- DOI: 10.7150/ijms.23525
Is pharmacologic treatment better than neural mobilization for cervicobrachial pain? A randomized clinical trial
Abstract
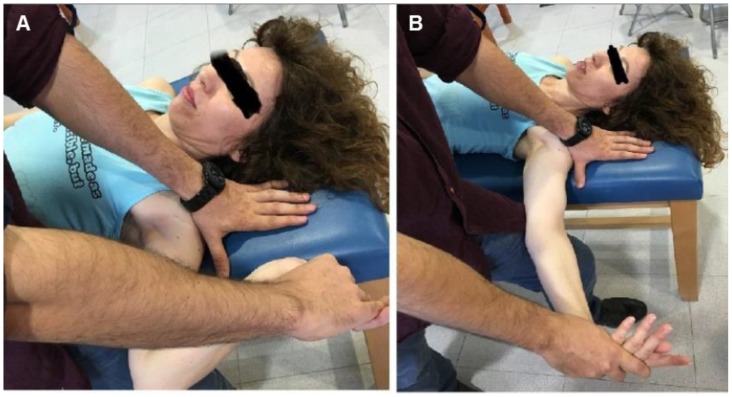
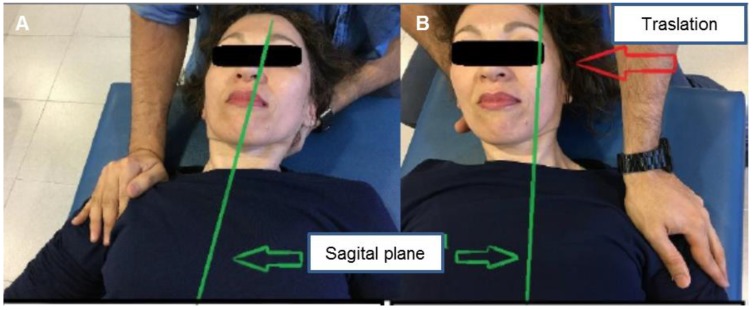
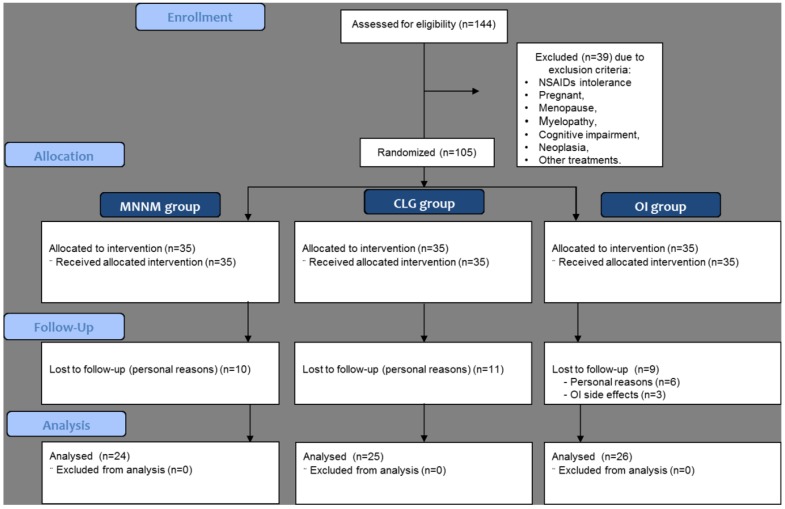
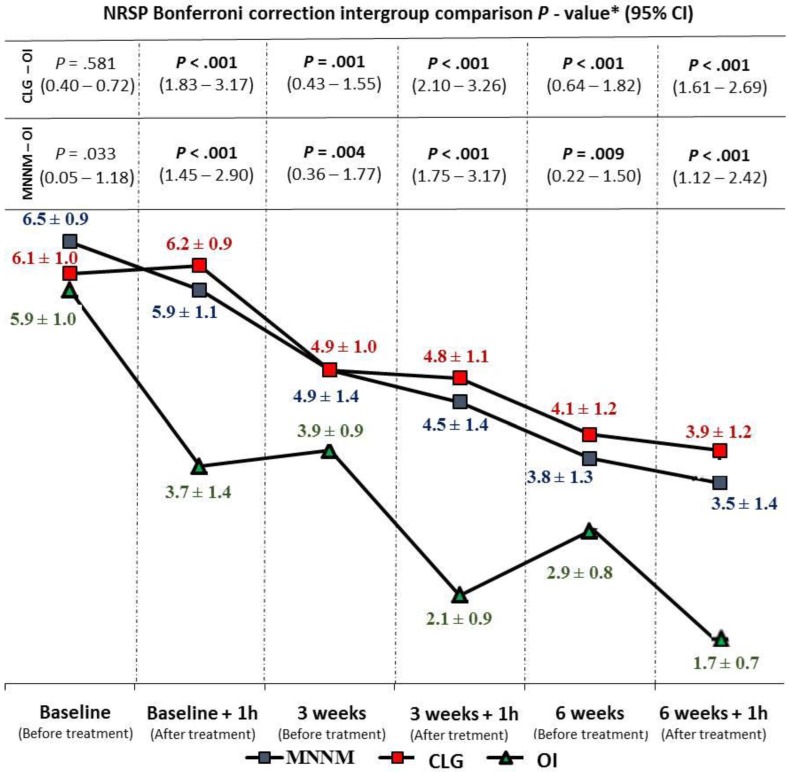
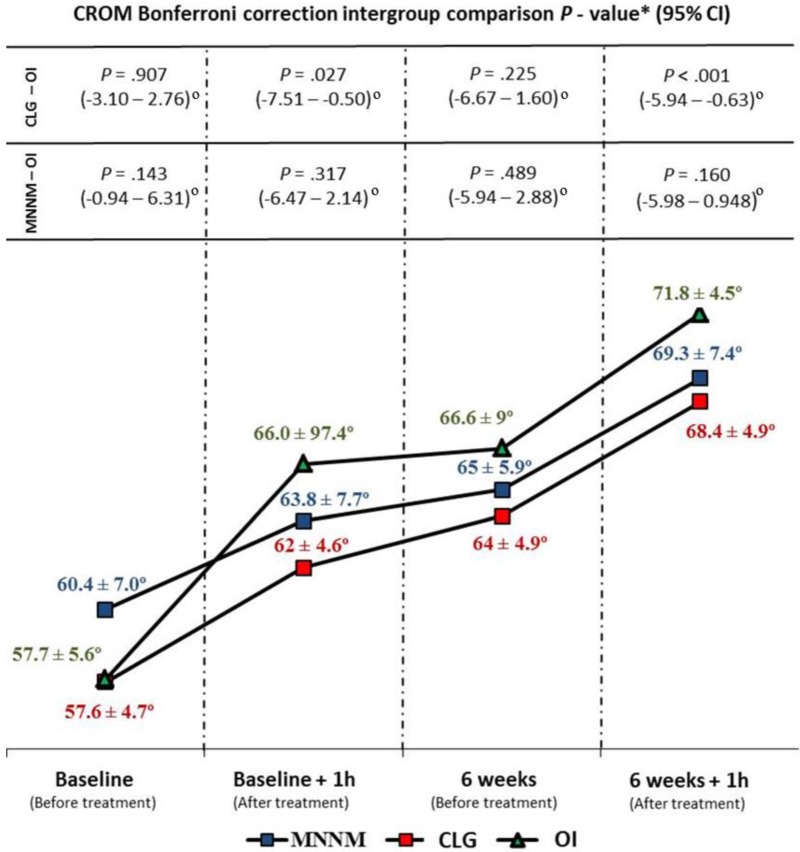
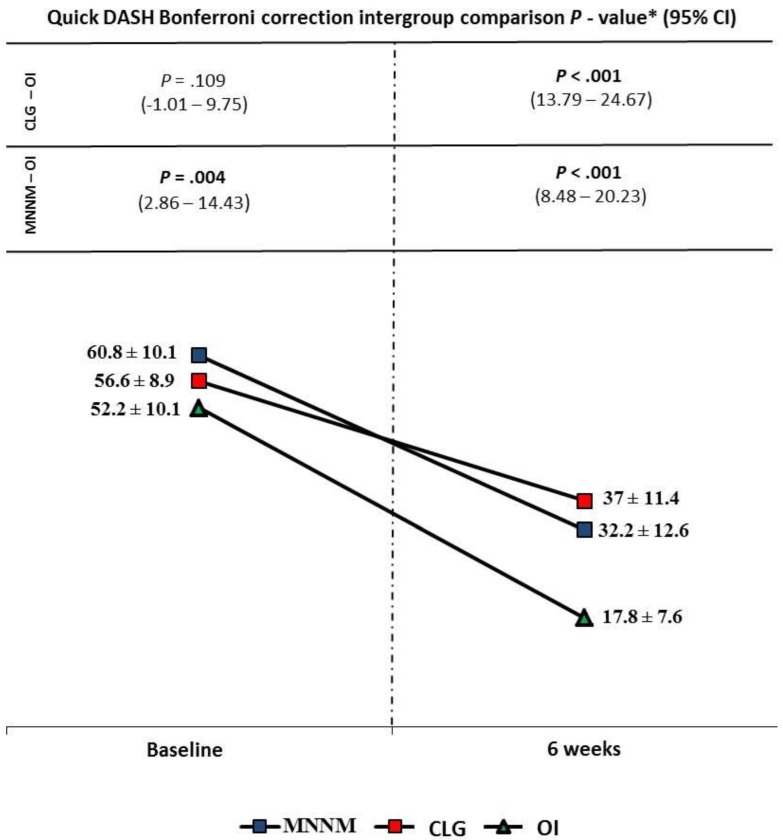
Purpose: This study aim was to compare the effectiveness of the median nerve neural mobilization (MNNM) and cervical lateral glide (CLG) intervention versus oral ibuprofen (OI) in subjects who suffer cervicobrachial pain (CP). Methods: This investigation was a, multicenter, blinded, randomized controlled clinical trial (NCT02595294; NCT02593721). A number of 105 individuals diagnosed with CP were enrolled in the study and treated in 2 different medical facilities from July to November 2015. Participants were recruited and randomly assigned into 3 groups of 35 subjects. Intervention groups received MNNM or CLG neurodynamic treatments, and the (active treatment) control group received an OI treatment for 6 weeks. Primary outcome was pain intensity reported through the Numeric Rating Scale for Pain (NRSP). Secondary outcomes were physical function involving the affected upper limb using the Quick DASH scale, and ipsilateral cervical rotation (ICR) using a cervical range of motion (CROM) device. Assessments were performed before and 1 hour after treatment for NRSP (baseline, 3 and 6 weeks) and CROM (baseline and 6 weeks), as well as only 1 assessment for Quick DASH (baseline and 6 weeks). Results: Repeated-measures ANOVA intergroup statistically significant differences were shown for CP intensity (F(2,72) = 22.343; P < .001; Eta2 = 0.383) and Quick DASH (F(2,72) = 15.338; P < .001; Eta2 = 0.299), although not for CROM (F(2,72) = 1.434; P = .245; Eta2 = 0.038). Indeed, Bonferroni´s correction showed statistically significant differences for CP intensity (P < .01; 95% CI = 0.22 - 3.26) and Quick DASH reduction (P < .01; 95% CI = 8.48 - 24.67) in favor of the OI treatment at all measurement moments after baseline. Conclusions: OI pharmacologic treatment may reduce pain intensity and disability with respect to neural mobilization (MNNM and CLG) in patients with CP during six weeks. Nevertheless, the non-existence of between-groups ROM differences and possible OI adverse effects should be considered.
Keywords: Musculoskeletal manipulations; Neck; Non-steroidal anti-inflammatory agents; Rehabilitation; Upper extremity..
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures
Similar articles
-
Cervical Lateral Glide Neural Mobilization Is Effective in Treating Cervicobrachial Pain: A Randomized Waiting List Controlled Clinical Trial.Pain Med. 2017 Dec 1;18(12):2492-2503. doi: 10.1093/pm/pnx011. Pain Med. 2017. PMID: 28340157 Clinical Trial.
-
Effects of Median Nerve Neural Mobilization in Treating Cervicobrachial Pain: A Randomized Waiting List-Controlled Clinical Trial.Pain Pract. 2018 Apr;18(4):431-442. doi: 10.1111/papr.12614. Epub 2017 Nov 20. Pain Pract. 2018. PMID: 28734105 Clinical Trial.
-
Effectiveness of median nerve neural mobilization versus oral ibuprofen treatment in subjects who suffer from cervicobrachial pain: a randomized clinical trial.Arch Med Sci. 2018 Jun;14(4):871-879. doi: 10.5114/aoms.2017.70328. Epub 2017 Sep 26. Arch Med Sci. 2018. PMID: 30002707 Free PMC article.
-
Immediate effects of cervicothoracic junction mobilization versus thoracic manipulation on the range of motion and pain in mechanical neck pain with cervicothoracic junction dysfunction: a pilot randomized controlled trial.Chiropr Man Therap. 2020 Aug 7;28(1):38. doi: 10.1186/s12998-020-00327-4. Chiropr Man Therap. 2020. PMID: 32762708 Free PMC article. Clinical Trial.
-
Effectiveness of Neural Mobilization Techniques in the Management of Musculoskeletal Neck Disorders with Nerve-Related Symptoms: A Systematic Review and Meta-Analysis with a Mapping Report.Pain Med. 2022 Apr 8;23(4):707-732. doi: 10.1093/pm/pnab300. Pain Med. 2022. PMID: 34633462
Cited by
-
Peripheral and central changes induced by neural mobilization in animal models of neuropathic pain: a systematic review.Front Neurol. 2024 Jan 5;14:1289361. doi: 10.3389/fneur.2023.1289361. eCollection 2023. Front Neurol. 2024. PMID: 38249743 Free PMC article.
-
Effects of neural mobilization of sciatic nerve and its branches in plantar foot pressures and stabilometry.Sci Rep. 2024 Oct 8;14(1):23417. doi: 10.1038/s41598-024-72848-4. Sci Rep. 2024. PMID: 39379413 Free PMC article. Clinical Trial.
-
The majority of clinical trials assessing mobilization and manipulation for neck pain lack a pragmatic approach: a systematic review of 174 trials.J Man Manip Ther. 2024 Oct;32(5):478-494. doi: 10.1080/10669817.2024.2327127. Epub 2024 Mar 25. J Man Manip Ther. 2024. PMID: 38525785 Free PMC article.
-
Quantifying the Elasticity Properties of the Median Nerve during the Upper Limb Neurodynamic Test 1.Appl Bionics Biomech. 2022 Mar 20;2022:3300835. doi: 10.1155/2022/3300835. eCollection 2022. Appl Bionics Biomech. 2022. PMID: 35355794 Free PMC article.
-
Atlasprofilax: a new promising treatment for chronic cervicobrachialgia. A qualitative-quantitative research of a retrospective longitudinal section, with a cause-effect approach.Front Med Technol. 2025 Mar 18;7:1513155. doi: 10.3389/fmedt.2025.1513155. eCollection 2025. Front Med Technol. 2025. PMID: 40171470 Free PMC article.
References
-
- Cleland JA, Whitman JM, Fritz JM, Palmer JA. Manual Physical Therapy, Cervical Traction, and Strengthening Exercises in Patients With Cervical Radiculopathy: A Case Series. J Orthop Sport Phys Ther. 2005;35:802–11. - PubMed
-
- Radhakrishnan K, Litchy WJ, O'Fallon WM, Kurland LT. Epidemiology of cervical radiculopathy. A population-based study from Rochester, Minnesota, 1976 through 1990. Brain. 1994;117:325–35. - PubMed
-
- Fisher RFG, Shaw PLF. Papiro quirúrgico de Edwin Smith. Historia y Filosofía de la Medicina. A Méd. 2005;50:43–8.
-
- Wagner SC, Van Blarcum GS, Kang DG, Lehman RA. Operative treatment of new onset radiculopathy secondary to combat injury. Mil Med. 2015;180:137–40. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
