

Intelligent Clinical Decision Support to Improve Safe Opioid Management of Chronic Noncancer Pain in Primary Care
- PMID: 29559866
- PMCID: PMC5855418
Intelligent Clinical Decision Support to Improve Safe Opioid Management of Chronic Noncancer Pain in Primary Care
Abstract
Background: Opioid prescription drug abuse is a major public health concern. Healthcare provider prescribing patterns, especially among non-pain management specialists, are a major factor. Practice guidelines recommend what to do for safe opioid prescribing but do not provide guidance on how to implement best practices.
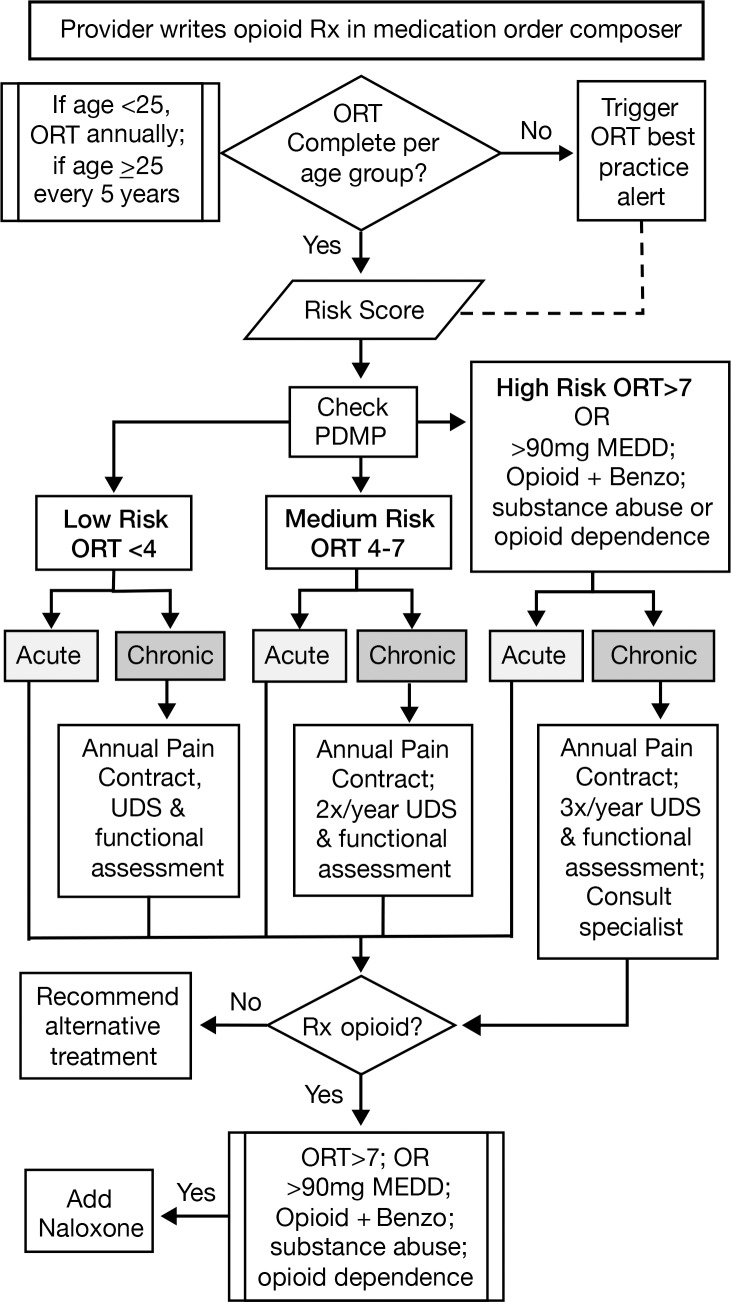
Methods: We describe the implementation of electronic medical record clinical decision support (EMR CDS) for opioid management of chronic noncancer pain in an integrated delivery system. This prospective cohort study will examine relationships between primary care physician compliance with EMR CDS-guided care (vs usual care), delivery of guideline-concordant care, and changes in the morphine equivalent of prescribed opioids. We report baseline characteristics of patients receiving chronic opioid therapy and organizational prescribing trends.
Results: Between August and October 2016, we identified 2,759 primary care patients who received chronic opioid therapy. Of these patients, approximately 71% had chronic noncancer pain, and 62% had diagnoses of depression/anxiety. Six of 36 primary care clinics each had >100 patients receiving chronic opioid therapy. When the EMR CDS launched in October 2017, we identified 54,200 patients who had received opioid therapy for at least 14 days from various specialty and primary care providers during the prior 24 months. Of these patients, 36% had a benzodiazepine coprescription, and 13% had substance abuse diagnoses.
Conclusion: Health system research that examines workflow-focused strategies to improve physician knowledge and skills for safely managing opioid therapy is needed. If EMR CDS proves to be effective in increasing adherence to practice guidelines, this EMR strategy can potentially be replicated and scaled up nationwide to improve population health management.
Keywords: Analgesics–opioid; chronic pain; decision support system–clinical; electronic medical records; primary health care.
Figures
References
-
- Quality improvement guidelines for the treatment of acute pain and cancer pain. American Pain Society Quality of Care Committee. JAMA. 1995. December 20; 274 23: 1874- 1880. - PubMed
-
- Manchikanti L., Abdi S., Atluri S., et al. American Society of Interventional Pain Physicians. American Society of Interventional Pain Physicians (ASIPP) guidelines for responsible opioid prescribing in chronic non-cancer pain: part 2—guidance. Pain Physician. 2012. July; 15 3 Suppl: S67- S116. - PubMed
-
- Centers for Disease Control and Prevention. Vital signs: overdoses of prescription opioid pain relievers—United States 1999-2008. MMWR Morb Mortal Wkly Rep. 2011. November 4; 60 43: 1487- 1492. - PubMed
LinkOut - more resources
Full Text Sources
Medical