

Cannabinoid Hyperemesis Syndrome: Public Health Implications and a Novel Model Treatment Guideline
- PMID: 29560069
- PMCID: PMC5851514
- DOI: 10.5811/westjem.2017.11.36368
Cannabinoid Hyperemesis Syndrome: Public Health Implications and a Novel Model Treatment Guideline
Abstract
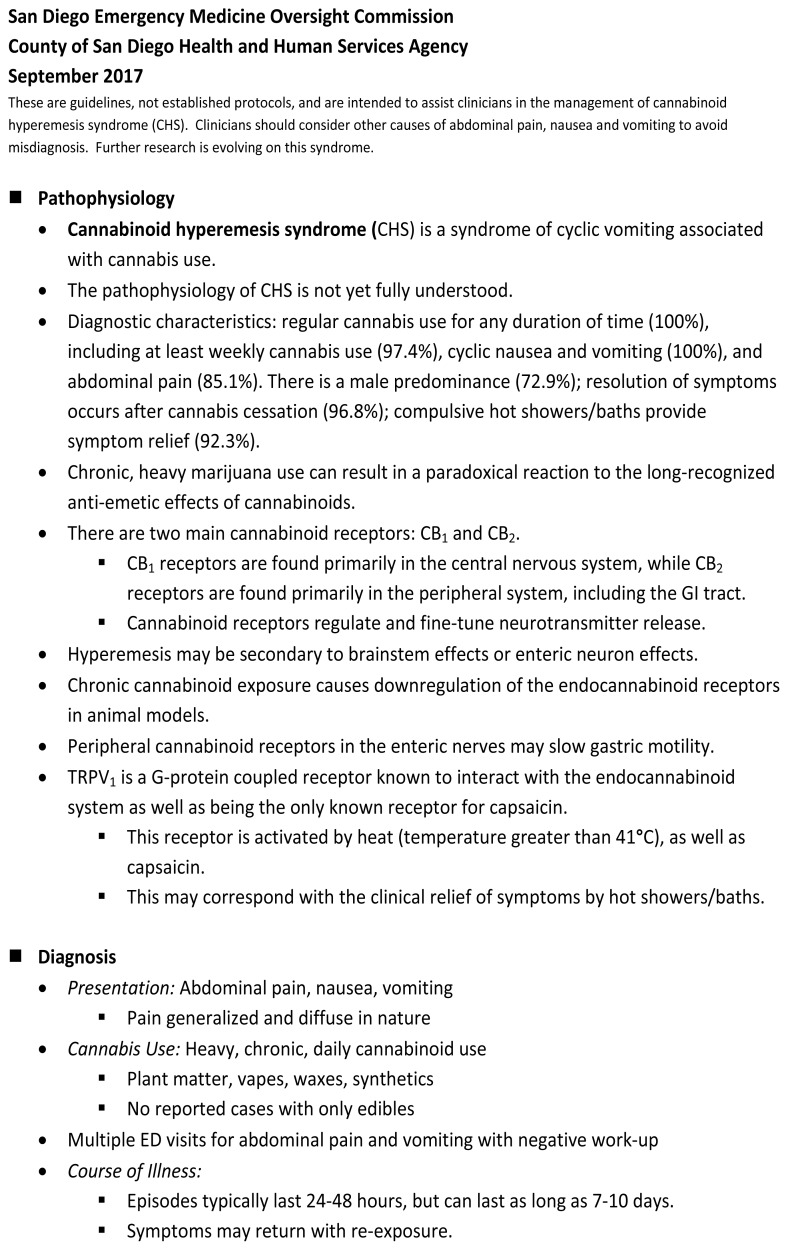
Introduction: Cannabinoid hyperemesis syndrome (CHS) is an entity associated with cannabinoid overuse. CHS typically presents with cyclical vomiting, diffuse abdominal pain, and relief with hot showers. Patients often present to the emergency department (ED) repeatedly and undergo extensive evaluations including laboratory examination, advanced imaging, and in some cases unnecessary procedures. They are exposed to an array of pharmacologic interventions including opioids that not only lack evidence, but may also be harmful. This paper presents a novel treatment guideline that highlights the identification and diagnosis of CHS and summarizes treatment strategies aimed at resolution of symptoms, avoidance of unnecessary opioids, and ensuring patient safety.
Methods: The San Diego Emergency Medicine Oversight Commission in collaboration with the County of San Diego Health and Human Services Agency and San Diego Kaiser Permanente Division of Medical Toxicology created an expert consensus panel to establish a guideline to unite the ED community in the treatment of CHS.
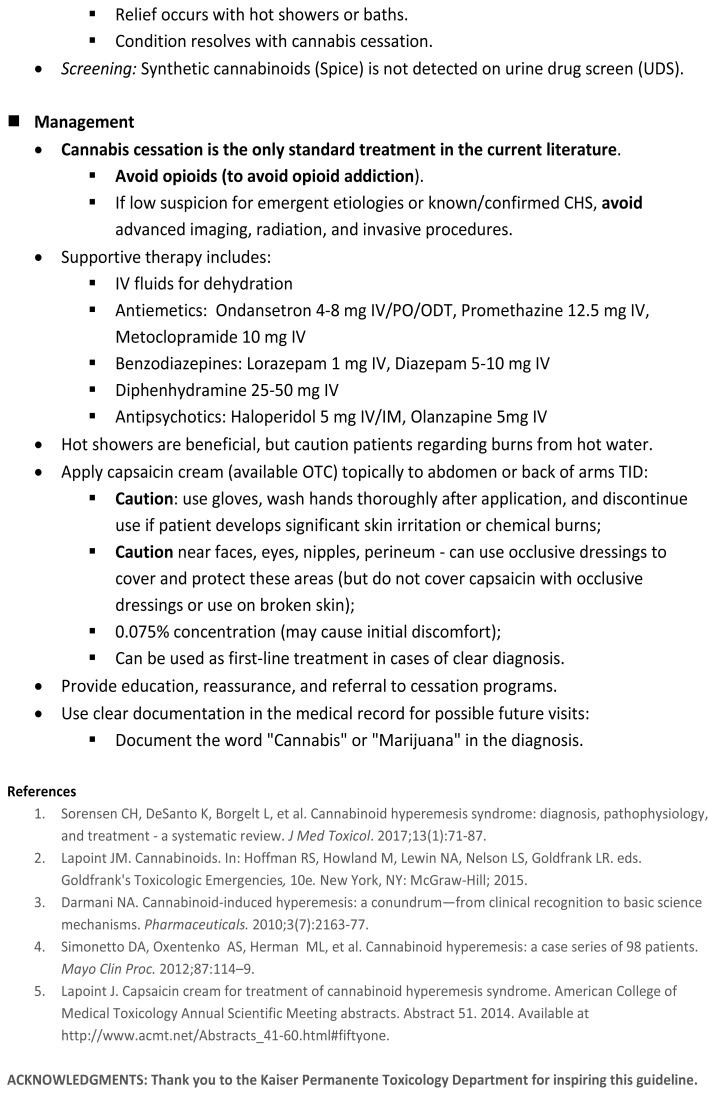
Results: Per the consensus guideline, treatment should focus on symptom relief and education on the need for cannabis cessation. Capsaicin is a readily available topical preparation that is reasonable to use as first-line treatment. Antipsychotics including haloperidol and olanzapine have been reported to provide complete symptom relief in limited case studies. Conventional antiemetics including antihistamines, serotonin antagonists, dopamine antagonists and benzodiazepines may have limited effectiveness. Emergency physicians should avoid opioids if the diagnosis of CHS is certain and educate patients that cannabis cessation is the only intervention that will provide complete symptom relief.
Conclusion: An expert consensus treatment guideline is provided to assist with diagnosis and appropriate treatment of CHS. Clinicians and public health officials should identity and treat CHS patients with strategies that decrease exposure to opioids, minimize use of healthcare resources, and maximize patient safety.
Conflict of interest statement
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. No author has professional or financial relationships with any companies that are relevant to this study. There are no conflicts of interest or sources of funding to declare.
Figures
References
-
- Results from the 2014 national survey on drug use and health: summary of national findings. [Accessed 4 April, 2017]. Available at: http://www.samhsa.gov/data.
-
- State medical marijuana laws. National Conference of State Legislatures. [Accessed 14 August, 2017]. Available at: http://www.ncsl.org/research/health/state-medical-marijuana-laws.aspx.
-
- 10 things to know about legal pot. CNN Money. [Accessed 14 August, 2017]. Available at: http://money.cnn.com/2017/04/19/news/legal-marijuana-420/index.html.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical