

Predictors of Mortality in Elder Patients With Proximal Humeral Fracture
- PMID: 29560284
- PMCID: PMC5851103
- DOI: 10.1177/2151458517728155
Predictors of Mortality in Elder Patients With Proximal Humeral Fracture
Abstract
Background: Known possible consequences of proximal humerus fractures include impaired shoulder function, decreased independence, and increased risk for mortality. The purpose of this report is to describe the survival and independence of elderly patients with fractures of the proximal humerus, treated in our institution, relative to patient characteristics and treatment method.
Methods: Retrospective cohort study from 2006 to 2012.
Setting: Community-based hospital with level 1 designation.
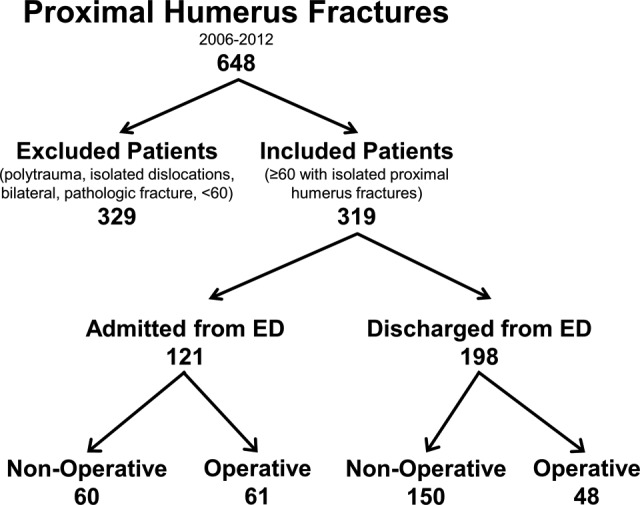
Patients/participants: Three hundred nineteen patients ≥60 years who presented to the emergency department with an isolated fracture of the proximal humerus were either admitted to the inpatient ward for the organization and provision of immediate definitive care or discharged with the expectation of coordination of their care as an outpatient. Treatment was nonoperative or operative.
Outcome measures: One- and 2-year mortality.
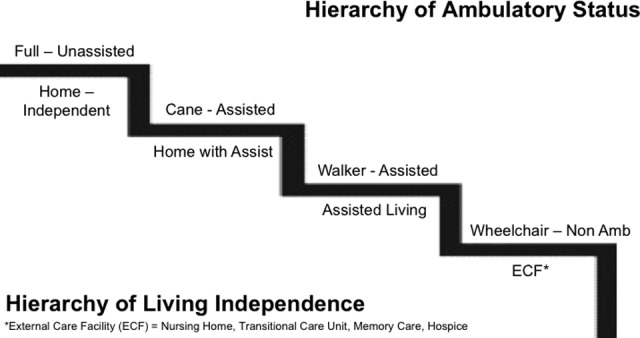
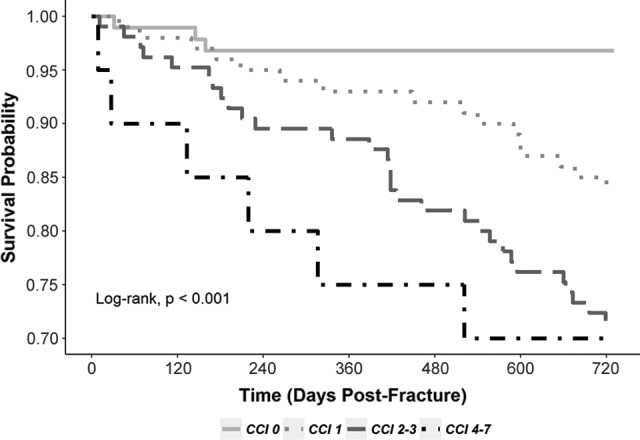
Results: Significant predictors of mortality at 1 year included Charlson Comorbidity Index (CCI; continuous, hazard ratio [HR] = 1.40; 95% confidence interval [CI]: 1.06-1.86), body mass index (BMI; <25 vs ≥25; HR = 3.43; 95% CI: 1.45-8.14), and American Society of Anesthesiologists (ASA) disease severity score (3-4 vs 1-2; HR = 4.48; 95% CI: 1.21-16.55). In addition to CCI and BMI, reliance on a cane/walker/wheelchair at the time of fracture predicted mortality at 2 years (vs unassisted ambulation; HR = 3.13; 95% CI: 1.59-5.88). Although the Neer classification of fracture severity significantly correlated with inpatient admission (P < .001), it was not significantly associated with mortality or with loss of living or ambulatory independence. Among admitted patients, 64% were discharged to a facility with a higher level of care than their prefracture living facility. Twenty percent of study patients experienced a loss in ambulatory status by at least 1 level at 1 year postfracture.
Conclusion: In a cohort of elderly patients with fractures of the proximal humerus, patient characteristics including comorbidities, ASA classification, and lower BMI were associated with increased mortality. Specifically, those admitted at the time of fracture and treated nonoperatively had the highest mortality rate and, likely, represent the frailest cohort. Those initially treated as outpatients and later treated operatively had the lowest mortality and, likely, represent the healthiest cohort. These data are inherently biased by prefracture comorbidities but help stratify our patients' mortality risk at the time of injury.
Keywords: fragility fractures; geriatric trauma; hospital admission; mortality; osteoporosis; proximal humerus fracture; trauma surgery; upper extremity surgery.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Court-Brown CM, McQueen MM. The relationship between fractures and increasing age with reference to the proximal humerus. The study of osteoporotic fractures research group. Curr Orthop. 2002;16(3):213–222.
-
- Kelsey JL, Browner WS, Seeley DG, Nevitt MC, Cummings SR. Risk factors for fractures of the distal forearm and proximal humerus. Am J Epidemiol. 1992;135(5):477–489. - PubMed
-
- Court-Brown CM, Garg A, McQueen MM. The epidemiology of proximal humeral fractures. Acta Orthop Scand. 2001;72(4):365–371. - PubMed
-
- Palvanen M, Kannus P, Niemi S, Parkkari J. Update in the epidemiology of proximal humeral fractures. Clin Ortho Relat Res. 2006;442:87–92. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
