

Evaluation of Statin Eligibility, Prescribing Practices, and Therapeutic Responses Using ATP III, ACC/AHA, and NLA Dyslipidemia Treatment Guidelines in a Large Urban Cohort of HIV-Infected Outpatients
- PMID: 29561173
- PMCID: PMC5808384
- DOI: 10.1089/apc.2017.0304
Evaluation of Statin Eligibility, Prescribing Practices, and Therapeutic Responses Using ATP III, ACC/AHA, and NLA Dyslipidemia Treatment Guidelines in a Large Urban Cohort of HIV-Infected Outpatients
Abstract
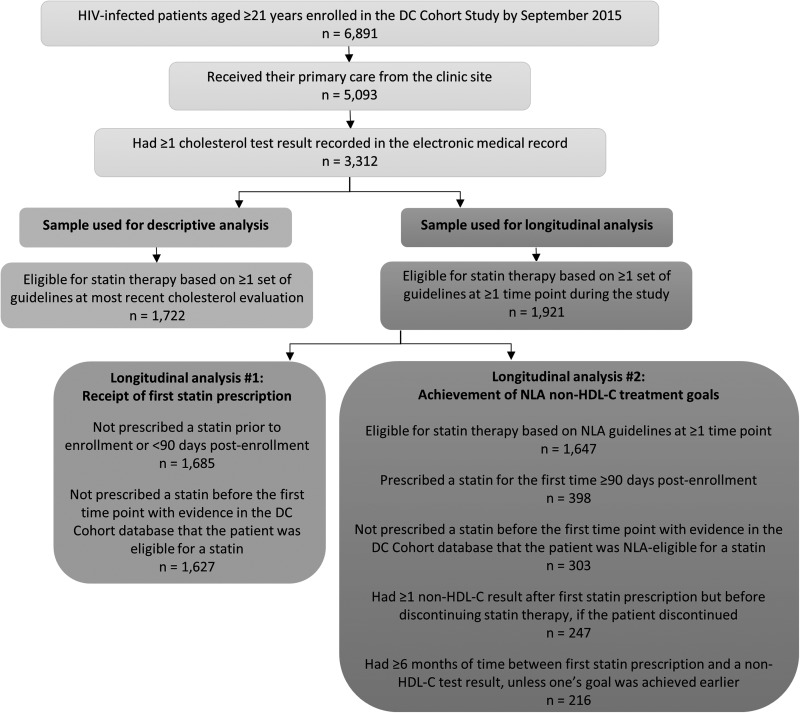
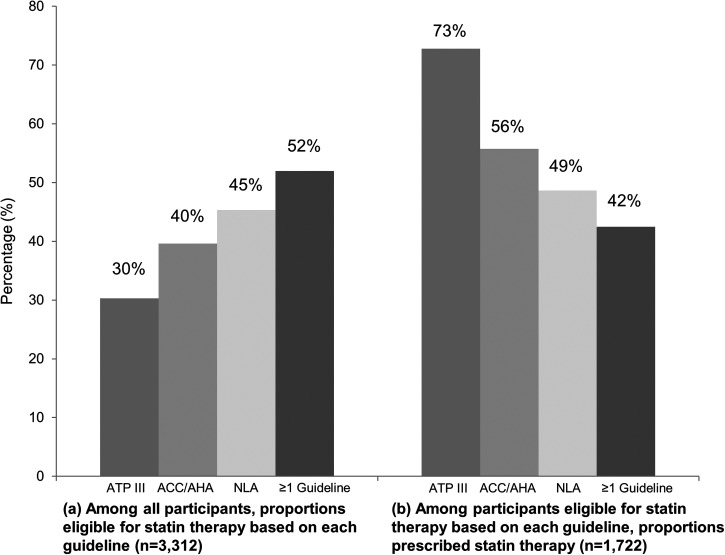
Statin coverage has been examined among HIV-infected patients using Adult Treatment Panel III (ATP III) and American College of Cardiology/American Heart Association (ACC/AHA) guidelines, although not with newer National Lipid Association (NLA) guidelines. We investigated statin eligibility, prescribing practices, and therapeutic responses using these three guidelines. Sociodemographic, clinical, and laboratory data were collected between 2011 and 2016 for HIV-infected outpatients enrolled in the DC Cohort, a multi-center, prospective, observational study in Washington, DC. This analysis included patients aged ≥21 years receiving primary care at their HIV clinic site with ≥1 cholesterol result available. Of 3312 patients (median age 52; 79% black), 52% were eligible for statins based on ≥1 guideline, including 45% (NLA), 40% (ACC/AHA), and 30% (ATP III). Using each guideline, 49% (NLA), 56% (ACC/AHA), and 73% (ATP III) of eligible patients were prescribed statins. Predictors of new prescriptions included older age (aHR = 1.16 [1.08-1.26]/5 years), body mass index ≥30 (aHR = 1.50 [1.07-2.11]), and diabetes (aHR = 1.35 [1.03-1.79]). Hepatitis C coinfection was inversely associated with statin prescriptions (aHR = 0.67 [0.45-1.00]). Among 216 patients with available cholesterol results pre-/post-prescription, 53% achieved their NLA cholesterol goal after 6 months. Hepatitis C coinfection was positively associated (aHR = 1.87 [1.06-3.32]), and depression (aHR = 0.56 [0.35-0.92]) and protease inhibitor use (aHR = 0.61 [0.40-0.93]) were inversely associated, with NLA goal achievement. Half of patients were eligible for statins based on current US guidelines, with the highest proportion eligible based on NLA guidelines, yet, fewer received prescriptions and achieved treatment goals. Greater compliance with recommended statin prescribing practices may reduce cardiovascular disease risk among HIV-infected individuals.
Keywords: HIV; cholesterol; dyslipidemia; guidelines; statins.
Conflict of interest statement
No conflicting financial interests exist.
Figures

References
-
- Martin-Iguacel R, Llibre JM, Friis-Moller N. Risk of cardiovascular disease in an aging HIV population: Where are we now? Curr HIV/AIDS Rep 2015;12:375–387 - PubMed
-
- Lee FJ, Carr A. Dyslipidemia in HIV-infected patients. In: Garg A, ed. Dyslipidemias: Pathophysiology, Evaluation and Management. New York: Humana Press, 2015;155–176
-
- Shahmanesh M, Schultze A, Burns F, et al. The cardiovascular risk management for people living with HIV in Europe: How well are we doing? AIDS 2016;30:2505–2518 - PubMed
-
- Friis-Moller N, Ryom L, Smith C, et al. An updated prediction model of the global risk of cardiovascular disease in HIV-positive persons: The Data-collection on Adverse Effects of Anti-HIV Drugs (D:A:D) study. Eur J Prev Cardiol 2016;23:214–223 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
