

A Review of the Impact of Obstetric Anesthesia on Maternal and Neonatal Outcomes
- PMID: 29561267
- PMCID: PMC6008182
- DOI: 10.1097/ALN.0000000000002182
A Review of the Impact of Obstetric Anesthesia on Maternal and Neonatal Outcomes
Abstract
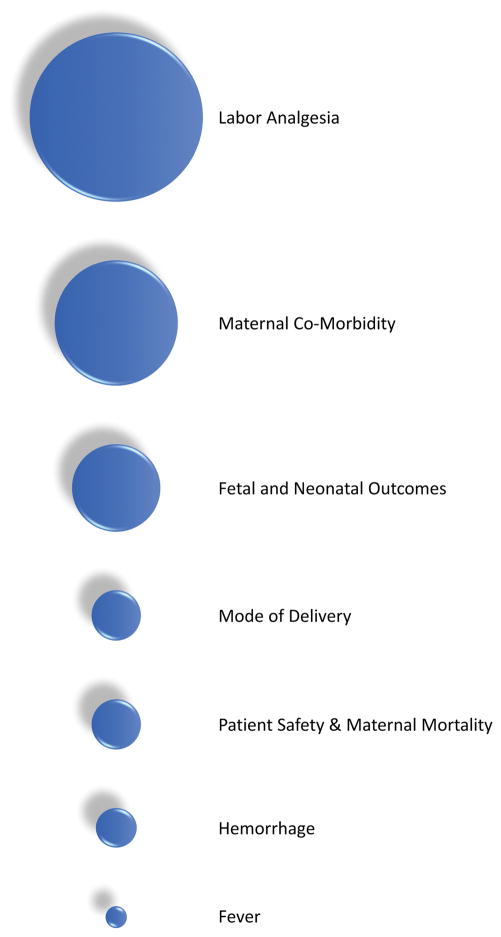
Obstetric anesthesia has evolved over the course of its history to encompass comprehensive aspects of maternal care, ranging from cesarean delivery anesthesia and labor analgesia to maternal resuscitation and patient safety. Anesthesiologists are concerned with maternal and neonatal outcomes, and with preventing and managing complications that may present during childbirth. The current review will focus on recent advances in obstetric anesthesia, including labor anesthesia and analgesia, cesarean delivery anesthesia and analgesia, the effects of maternal anesthesia on breastfeeding and fever, and maternal safety. The impact of these advances on maternal and neonatal outcomes is discussed. Past and future progress in this field will continue to have significant implications on the health of women and children.
Conflict of interest statement
Figures
References
-
- Caton D. John Snow’s practice of obstetric anesthesia. Anesthesiology. 2000;92:247–52. - PubMed
-
- Caton D. The influence of social values on obstetric anesthesia. AMA J Ethics. 2015;17:253–7. - PubMed
-
- Mendelson CL. The aspiration of stomach contents into the lungs during obstetric anesthesia. Am J Obstet Gynecol. 1946;52:191–205. - PubMed
-
- Thorp JA, Hu DH, Albin RM, McNitt J, Meyer BA, Cohen GR, Yeast JD. The effect of intrapartum epidural analgesia on nulliparous labor: a randomized, controlled, prospective trial. Am J Obstet Gynecol. 1993;169:851–8. - PubMed
-
- Hawkins JL, Chang J, Palmer SK, Gibbs CP, Callaghan WM. Anesthesia-related maternal mortality in the United States: 1979–2002. Obstet Gynecol. 2011;117:69–74. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
