

The Management of Critically Colonized and Locally Infected Leg Ulcers with an Acid-Oxidizing Solution: A Pilot Study
- PMID: 29561341
- PMCID: PMC5895123
- DOI: 10.1097/01.ASW.0000530687.23867.bd
The Management of Critically Colonized and Locally Infected Leg Ulcers with an Acid-Oxidizing Solution: A Pilot Study
Abstract
Objective: Critical colonization or local infection is very common in chronic wounds, but clinically problematic. Because therapeutic options for these conditions are limited in number and efficacy, the study authors tested a new acid-oxidizing solution (AOS [Nexodyn]; APR Applied Pharma Research S.A., Balerna, Switzerland) to determine its ancillary antimicrobial properties and potential support for wound healing.
Design and setting: This open-label clinical case series was conducted with a prospective, single-arm design at the Federal County Hospital in Bregenz, Austria.
Patients: In the study, 30 patients with critically colonized or locally infected chronic leg ulcers of any origin were included.
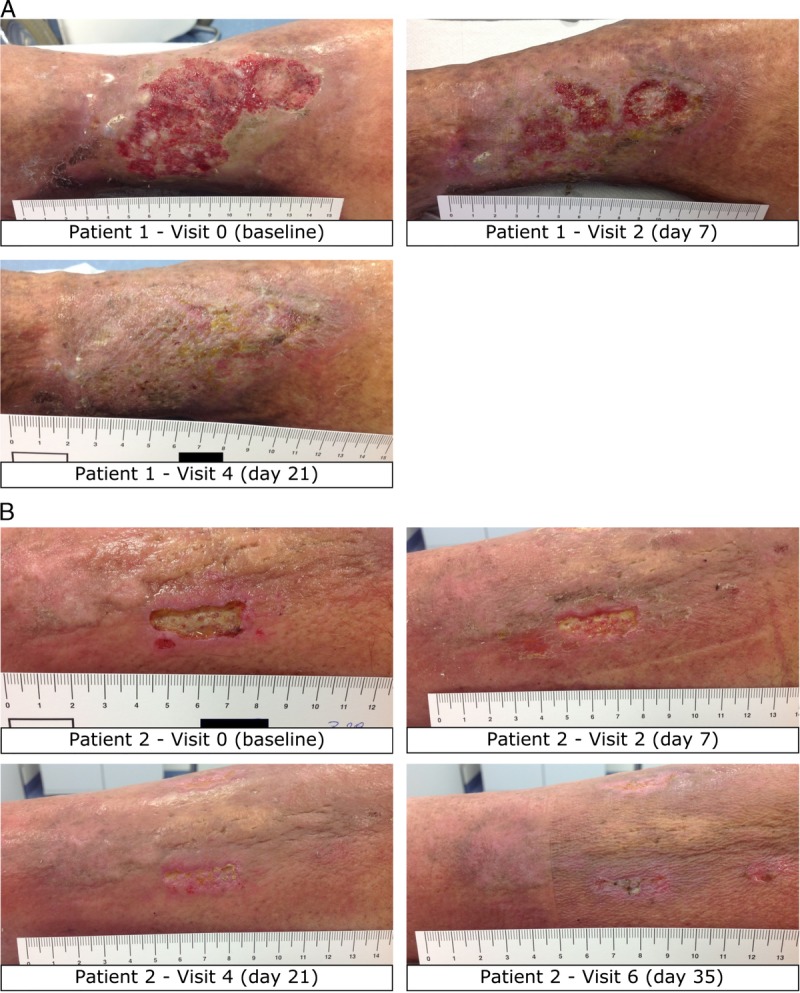
Interventions: The AOS was applied on each leg ulcer at every dressing change for 35 days.
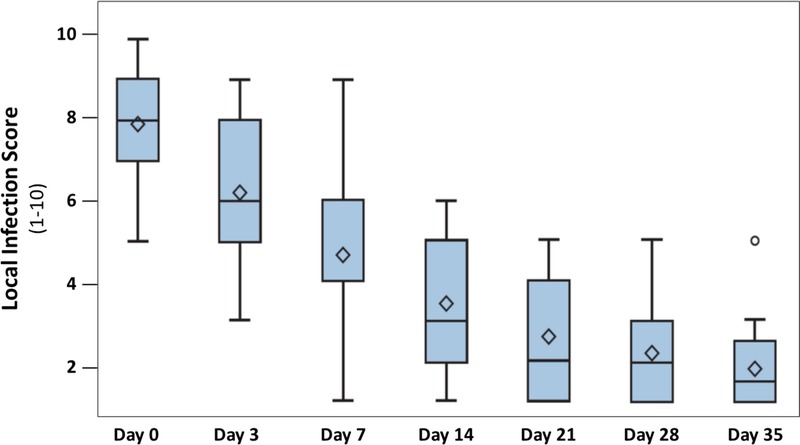
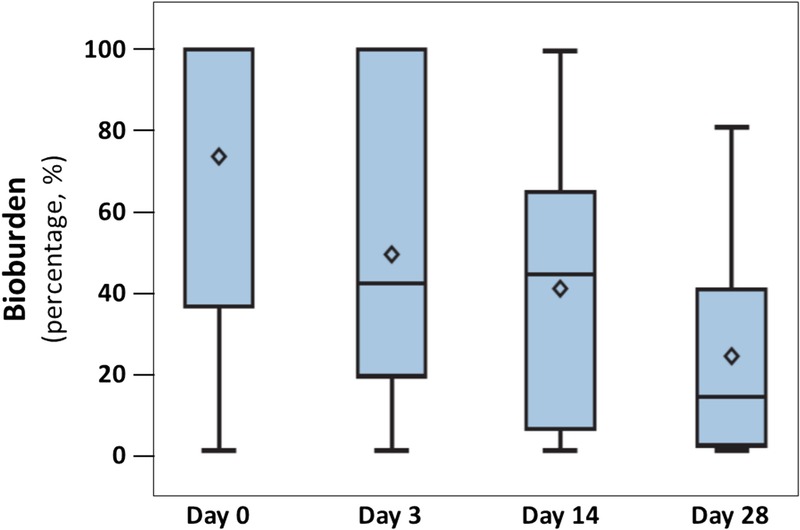
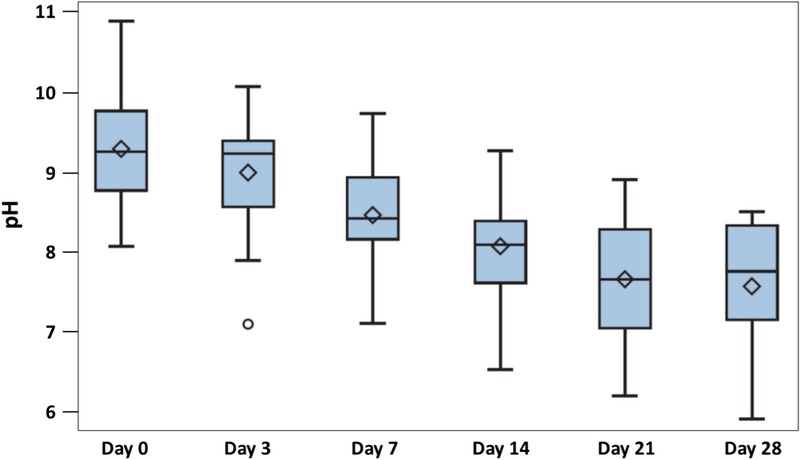
Main outcome measures: The tolerability and performance of the AOS were assessed by evaluating the ulcer characteristics and comparing them with those at baseline. The clinical course of wounds was analyzed using standard measures for bioburden, local infection, pain, pH, and wound healing.
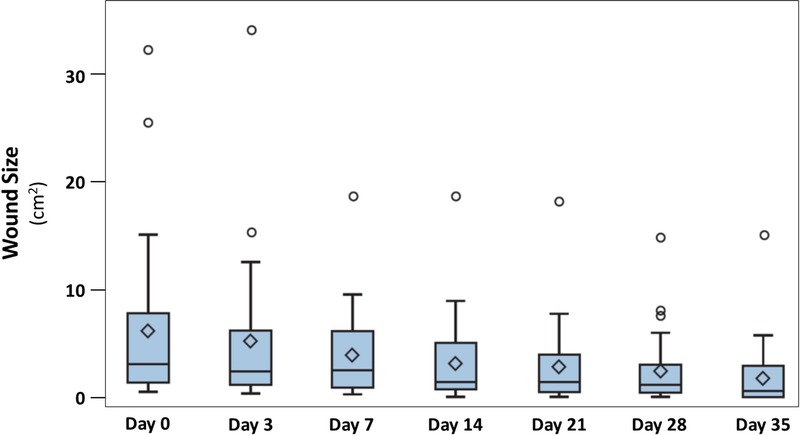
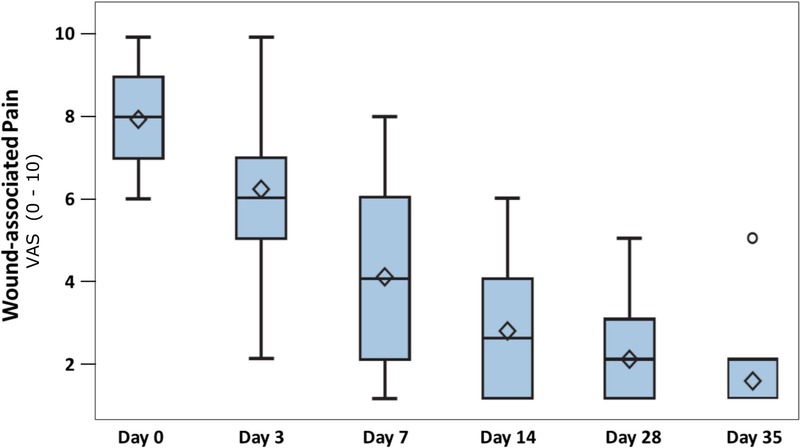
Main results: Application of the solution was well tolerated, and no adverse events were recorded. In all patients, local infection was overcome, and wound bed pH and wound area decreased significantly. In addition, patient pain levels decreased to a level where interventions were not required after study day 7. In 37% of all patients, a complete resolution of chronic ulcers was achieved by the end of the study period.
Conclusion: According to these results, the AOS seems to be a valid and highly tolerable treatment to support wound healing in locally infected ulcers. Nevertheless, larger controlled cohort studies are needed to substantiate these findings.
Conflict of interest statement
The other authors declare that they have no conflicts of interest.
Figures
References
-
- Valencia IC, Falabella A, Kirsner RS, Eaglstein WH. Chronic venous insufficiency and venous leg ulceration. J Am Acad Dermatol 2001;44(3):401-21. - PubMed
-
- Richmond NA, Maderal AD, Vivas AC. Evidence-based management of common chronic lower extremity ulcers. Dermatol Ther 2013;26(3):187-96. - PubMed
-
- Rayner R, Carville K, Keaton J, Prentice J, Santamaria N. Leg ulcers: atypical presentations and associated comorbidities. Wound Pract Res 2009;17(4):168-85.
-
- Agale SV. Chronic leg ulcers: epidemiology, aetiopathogenesis, and management. Ulcers 2013;2013:1-9.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
