

Rupture of multiple pseudoaneurysms as a rare complication of common iliac artery balloon occlusion in a patient with placenta accreta: A case report and review of literature
- PMID: 29561462
- PMCID: PMC5895301
- DOI: 10.1097/MD.0000000000009896
Rupture of multiple pseudoaneurysms as a rare complication of common iliac artery balloon occlusion in a patient with placenta accreta: A case report and review of literature
Abstract
Rationale: Placenta accreta is the main cause of severe obstetric postpartum hemorrhage (PPH) and hysterectomy. Several hemostatic techniques have been performed in patients with placenta accreta to prevent PPH and reserve fertility. Abdominal aorta and pelvic arteries balloon occlusion are the only techniques which could be performed before cesarean section (CS) in patients who want to keep the fetus and reserve fertility. However, abdominal aorta and pelvic arteries balloon occlusion might lead to severe complications such as formation and rupture of pseudoaneurysm, angiorrhexis, etc.
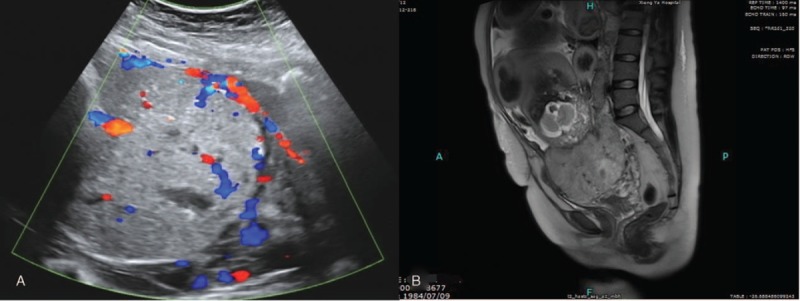
Patient concerns: We report a case diagnosed with pernicious placenta previa (PPP) combined with Rh(D) negative blood type, who was performed with bilateral common iliac arteries (CIA) balloon occlusion during CS. However, on the first day after CS, the patient caught sudden left-side lumbago and backache accompanied with palpitation and shortness of breath.
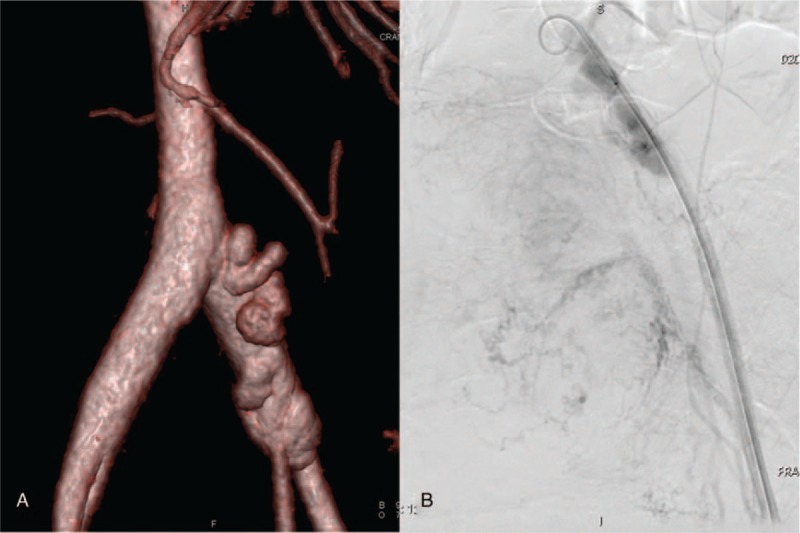
Diagnoses: Formation and rupture of multiple pseudoaneurysms in left CIA.
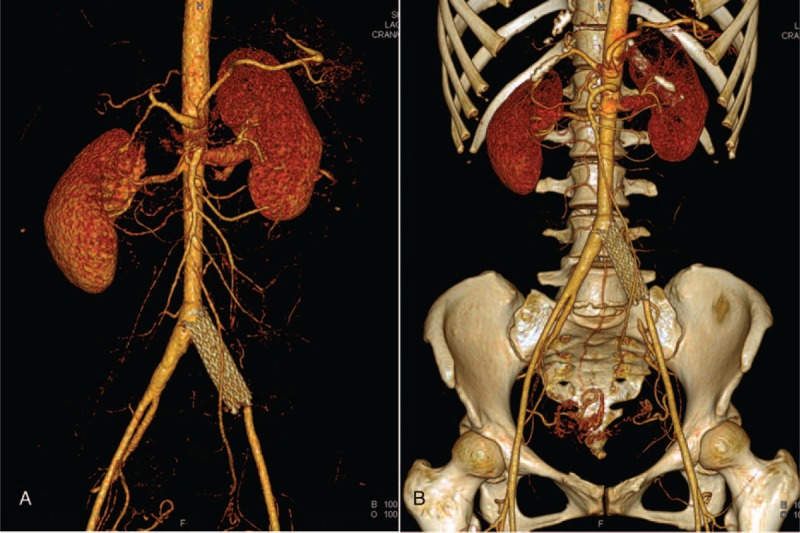
Interventions: Covered stent was inserted into the proximal part of the left CIA and the ipsilateral internal iliac artery was embolized by coil to prevent endoleak.
Outcomes: The patient recovered and discharged from hospital in stable condition without other complications 9 days after CS.
Lessons: It is of paramount importance that obstetricians and radiologists correctly estimate the appropriate occlusion volume and pressure of pelvic arteries before CS to avoid formation and rupture of a pseudoaneurysm. And if the rupture of a pseudoaneurysm occurred, it should be quickly identified and treated with endovascular intervention.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Safety and Efficacy of Aortic Vs Internal Iliac Balloon Occlusion for Cesarean Delivery in Coexisting Placenta Accreta and Placenta Previa.Cardiovasc Intervent Radiol. 2020 Sep;43(9):1277-1284. doi: 10.1007/s00270-020-02548-9. Epub 2020 Jun 12. Cardiovasc Intervent Radiol. 2020. PMID: 32533311
-
Prophylactic balloon occlusion of internal iliac arteries, common iliac arteries and infrarenal abdominal aorta in pregnancies complicated by placenta accreta: a retrospective cohort study.Eur Radiol. 2018 Dec;28(12):4959-4967. doi: 10.1007/s00330-018-5527-7. Epub 2018 Jun 5. Eur Radiol. 2018. PMID: 29872910
-
Effect of prophylactic balloon occlusion of internal iliac artery in pregnancies complicated by placenta previa and accreta.BMC Pregnancy Childbirth. 2021 Sep 21;21(1):640. doi: 10.1186/s12884-021-04103-x. BMC Pregnancy Childbirth. 2021. PMID: 34548060 Free PMC article.
-
The effect prophylactic internal iliac artery balloon occlusion in patients with placenta previa or placental accreta spectrum: a systematic review and meta-analysis.Reprod Biol Endocrinol. 2021 Mar 4;19(1):40. doi: 10.1186/s12958-021-00722-3. Reprod Biol Endocrinol. 2021. PMID: 33663536 Free PMC article.
-
Treatment of infected placenta accreta in the uterine horn by transabdominal temporary occlusion of internal iliac arteries: A case report and literature review.Medicine (Baltimore). 2023 Aug 11;102(32):e34525. doi: 10.1097/MD.0000000000034525. Medicine (Baltimore). 2023. PMID: 37565879 Free PMC article. Review.
Cited by
-
Same Clinical Reality of Spontaneous Rupture of the Common Iliac Artery with Pseudoaneurysm Formation-Comparison of Two Therapeutical Solutions, Endovascular Stent-Graft and Open Surgical Correction, for Two Cases and Review of the Literature.J Clin Med. 2023 Jan 16;12(2):713. doi: 10.3390/jcm12020713. J Clin Med. 2023. PMID: 36675646 Free PMC article.
-
Role of Abdominal Aortic Balloon Placement in Planned Conservative Management of Placenta Previa With Placenta Increta or Percreta.Front Med (Lausanne). 2021 Dec 14;8:767748. doi: 10.3389/fmed.2021.767748. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34970561 Free PMC article.
-
The role of interventional radiology in the management of abnormally invasive placenta: a systematic review of current evidences.Quant Imaging Med Surg. 2020 Jun;10(6):1370-1391. doi: 10.21037/qims-20-548. Quant Imaging Med Surg. 2020. PMID: 32550143 Free PMC article. Review.
-
Perioperative patient blood management during parallel transverse uterine incision cesarean section in patient with pernicious placenta previa: A retrospective cohort analysis.Medicine (Baltimore). 2020 Aug 28;99(35):e21916. doi: 10.1097/MD.0000000000021916. Medicine (Baltimore). 2020. PMID: 32871925 Free PMC article.
-
Placenta Accreta Spectrum Outcomes Using Tourniquet and Forceps for Vascular Control.Front Med (Lausanne). 2021 Oct 18;8:557678. doi: 10.3389/fmed.2021.557678. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34733857 Free PMC article.
References
-
- Silver RM. Abnormal placentation: placenta previa, vasa previa, and placenta accreta. Obstet Gynecol 2015;126:654–68. - PubMed
-
- Peng Q, Zhang W. Uterine arterial embolization to assist induction of labor among patients with complete placenta previa. Int J Gynaecol Obstet 2015;130:132–6. - PubMed
-
- Duan XH, Wang YL, Han XW, et al. Caesarean section combined with temporary aortic balloon occlusion followed by uterine artery embolisation for the management of placenta accreta. Clin Radiol 2015;70:932–7. - PubMed
-
- Sewell MF, Rosenblum D, Ehrenberg H. Arterial embolus during common iliac balloon catheterization at cesarean hysterectomy. Obstet Gynecol 2006;108:746–8. - PubMed
-
- Carnevale FC, Kondo MM, de Oliveira Sousa W, Jr, et al. Perioperative temporary occlusion of the internal iliac arteries as prophylaxis in cesarean section at risk of hemorrhage in placenta accreta. Cardiovasc Intervent Radiol 2011;34:758–64. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
