

Association of Frailty With Failure to Rescue After Low-Risk and High-Risk Inpatient Surgery
- PMID: 29562073
- PMCID: PMC5875343
- DOI: 10.1001/jamasurg.2018.0214
Association of Frailty With Failure to Rescue After Low-Risk and High-Risk Inpatient Surgery
Abstract
Importance: Failure to rescue (FTR), or death after a potentially preventable complication, is a nationally endorsed, publicly reported quality measure. However, little is known about the impact of frailty on FTR, in particular after low-risk surgical procedures.
Objective: To assess the association of frailty with FTR in patients undergoing inpatient surgery.
Design, setting, and participants: This study assessed a cohort of 984 550 patients undergoing inpatient general, vascular, thoracic, cardiac, and orthopedic surgery in the National Surgical Quality Improvement Program between January 1, 2005, and December 31, 2012. Frailty was assessed using the Risk Analysis Index (RAI), and patients were stratified into 5 groups (RAI score, ≤10, 11-20, 21-30, 31-40, and >40). Procedures were categorized as low mortality risk (≤1%) or high mortality risk (>1%). The association between RAI scores, the number of postoperative complications (0, 1, 2, or 3 or more), and FTR was evaluated using hierarchical modeling.
Main outcomes and measures: The number of postoperative complications and inpatient FTR.
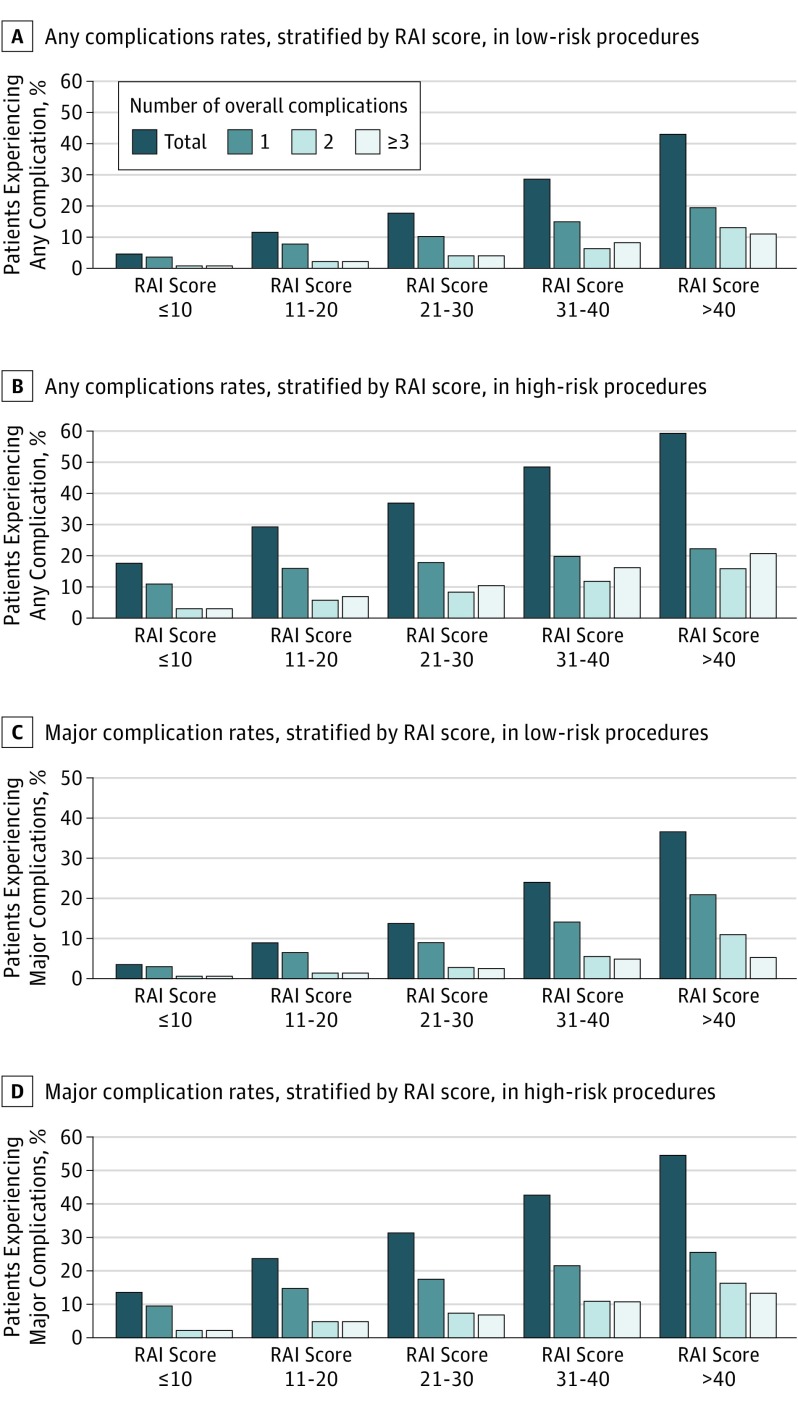
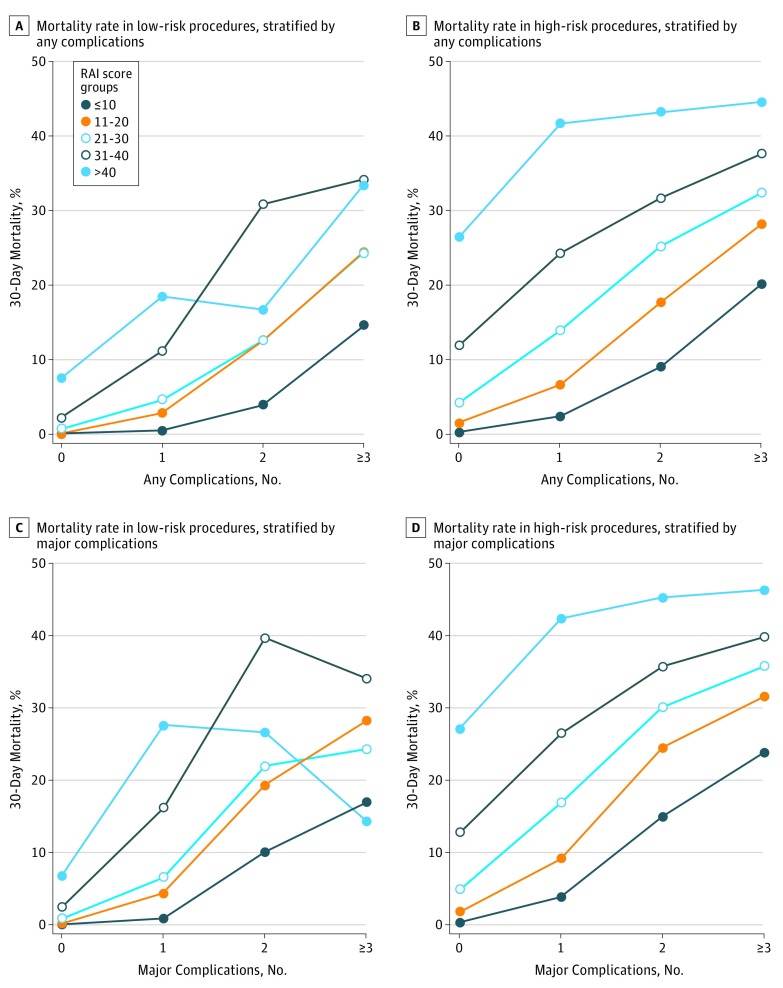
Results: A total of 984 550 patients were included, with a mean (SD) age of 58.2 (17.1) years; women were 549 281 (55.8%) of the cohort. For patients with RAI scores of 10 or less, major complication rates after low-risk surgery were 3.2%; rates of those with RAI scores of 11 to 20, 21 to 30, 31 to 40, and more than 40 were 8.6%, 13.5%, 23.8%, and 36.4%, respectively. After high-risk surgery, these rates were 13.5% for those with scores of 10 or less, 23.7% for those with scores of 11 to 20, 31.1% for those with scores of 21 to 30, 42.5% for those with scores of 31 to 40, and 54.4% for those with scores of more than 40. Stratifying by the number of complications, significant increases in FTR were observed across RAI categories after both low-risk and high-risk procedures. After a low-risk procedure, odds of FTR after 1 major complication for patients with RAI scores of 11 to 20 increased 5-fold over those with RAI scores of 10 or less (odds ratio [OR], 5.3; 95% CI, 3.9-7.1). Odds ratios were 8.1 (95% CI, 5.6-11.7) for patients with RAI scores of 21 to 30; 22.3 (95% CI, 13.9-35.6) for patients with scores of 31 to 40; and 43.9 (95% CI, 19-101.1) for patients with scores of more than 40. For patients undergoing a high-risk procedure, the corresponding ORs were likewise consistently elevated (RAI score 11-20: OR, 2.5; 95% CI, 2.3-2.7; vs RAI score 21-30: 5.1; 95% CI, 4.6-5.5; vs RAI score 31-40: 8.9; 95% CI, 8.1-9.9; vs RAI score >40: 18.4; 95% CI, 15.7-21.4).
Conclusions and relevance: Frailty has a dose-response association with complications and FTR, which is apparent after low-risk and high-risk inpatient surgery. Systematic assessment of frailty in preoperative patients may help refine estimates of surgical risk that could identify patients who might benefit from perioperative interventions designed to enhance physiologic reserve and potentially mitigate aspects of procedural risk, and would provide a framework for shared decision-making regarding the value of a given surgical procedure.
Conflict of interest statement
Figures
Comment in
-
From Preoperative Assessment to Preoperative Optimization of Frailty.JAMA Surg. 2018 May 16;153(5):e180213. doi: 10.1001/jamasurg.2018.0213. Epub 2018 May 16. JAMA Surg. 2018. PMID: 29562059 No abstract available.
References
-
- Colby SL, Ortman JM; United States Census Bureau Projections of the size and composition of the US population 2014 to 2060: population estimates and projections: current population reports. https://census.gov/content/dam/Census/library/publications/2015/demo/p25.... Published March 2015. Accessed February 15, 2018.
-
- Fried LP, Ferrucci L, Darer J, Williamson JD, Anderson G. Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. J Gerontol A Biol Sci Med Sci. 2004;59(3):-. - PubMed
-
- Kelaiditi E, Cesari M, Canevelli M, et al. ; IANA/IAGG . Cognitive frailty: rational and definition from an (IANA/IAGG) international consensus group. J Nutr Health Aging. 2013;17(9):726-734. - PubMed
-
- Makary MA, Segev DL, Pronovost PJ, et al. Frailty as a predictor of surgical outcomes in older patients. J Am Coll Surg. 2010;210(6):901-908. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
