

Altered metabolism distinguishes high-risk from stable carotid atherosclerotic plaques
- PMID: 29562241
- PMCID: PMC6012762
- DOI: 10.1093/eurheartj/ehy124
Altered metabolism distinguishes high-risk from stable carotid atherosclerotic plaques
Abstract
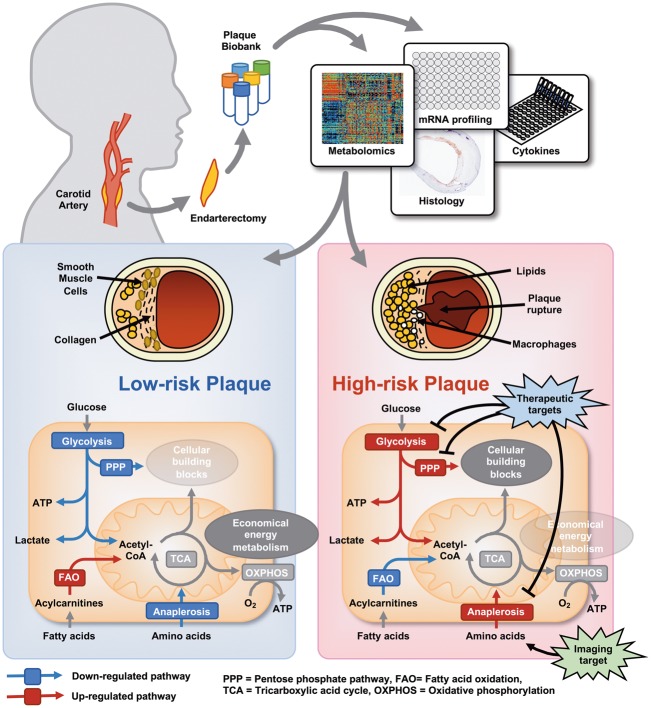
Aims: Identification and treatment of the rupture prone atherosclerotic plaque remains a challenge for reducing the burden of cardiovascular disease. The interconnection of metabolic and inflammatory processes in rupture prone plaques is poorly understood. Herein, we investigate associations between metabolite profiles, inflammatory mediators and vulnerability in carotid atherosclerotic plaques.
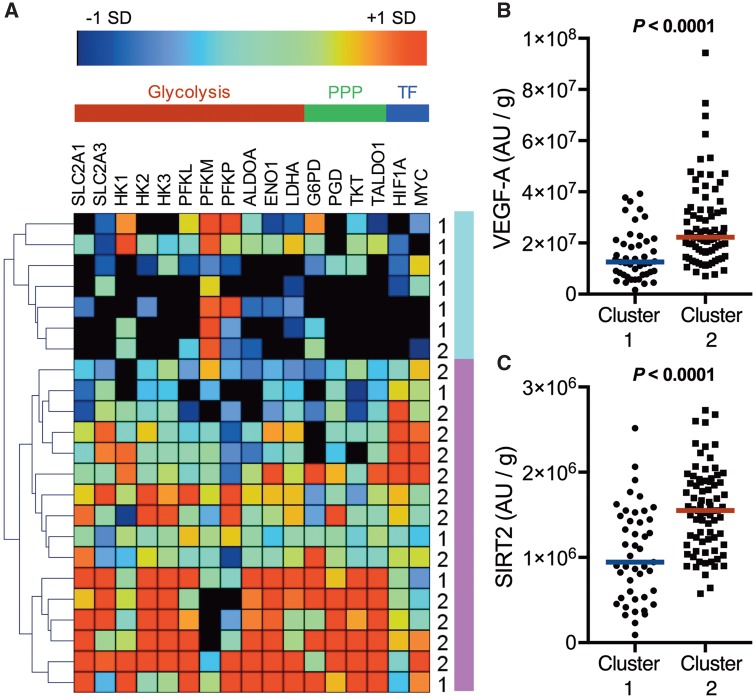
Methods and results: We collected 159 carotid plaques from patients undergoing endarterectomy and measured 165 different metabolites in a targeted metabolomics approach. We identified a metabolite profile in carotid plaques that associated with histologically evaluated vulnerability and inflammatory mediators, as well as presence of symptoms in patients. The distinct metabolite profiles identified in high-risk and stable plaques were in line with different transcription levels of metabolic enzymes in the two groups, suggesting an altered metabolism in high-risk plaques. The altered metabolic signature in high-risk plaques was consistent with a change to increased glycolysis, elevated amino acid utilization and decreased fatty acid oxidation, similar to what is found in activated leucocytes and cancer cells.
Conclusion: These results highlight a possible key role of cellular metabolism to support inflammation and a high-risk phenotype of atherosclerotic plaques. Targeting the metabolism of atherosclerotic plaques with novel metabolic radiotracers or inhibitors might therefore be valid future approaches to identify and treat the high-risk atherosclerotic plaque.
Figures



Comment in
-
Metabolomic profiling of atherosclerotic plaques: towards improved cardiovascular risk stratification.Eur Heart J. 2018 Jun 21;39(24):2311-2313. doi: 10.1093/eurheartj/ehy117. Eur Heart J. 2018. PMID: 29562256 No abstract available.
References
-
- Nilsson J. Atherosclerotic plaque vulnerability in the statin era. Eur Heart J 2017;38:1638–1644. - PubMed
-
- Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med 2005;352:1685–1695. - PubMed
-
- North American Symptomatic Carotid Endarterectomy Trial Collaborators. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. N Engl J Med 1991;325:445–453. - PubMed
-
- European Carotid Surgery Trialists Collaborative Group. Risk of stroke in the distribution of an asymptomatic carotid artery. The European Carotid Surgery Trialists Collaborative Group. Lancet 1995;345:209–212. - PubMed
-
- Hellings WE, Peeters W, Moll FL, Piers SR, van Setten J, van der Spek PJ, de Vries JP, Seldenrijk KA, De Bruin PC, Vink A, Velema E, de Kleijn DP, Pasterkamp G.. Composition of carotid atherosclerotic plaque is associated with cardiovascular outcome: a prognostic study. Circulation 2010;121:1941–1950. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
