

Profiling walking dysfunction in multiple sclerosis: characterisation, classification and progression over time
- PMID: 29563533
- PMCID: PMC5862880
- DOI: 10.1038/s41598-018-22676-0
Profiling walking dysfunction in multiple sclerosis: characterisation, classification and progression over time
Abstract
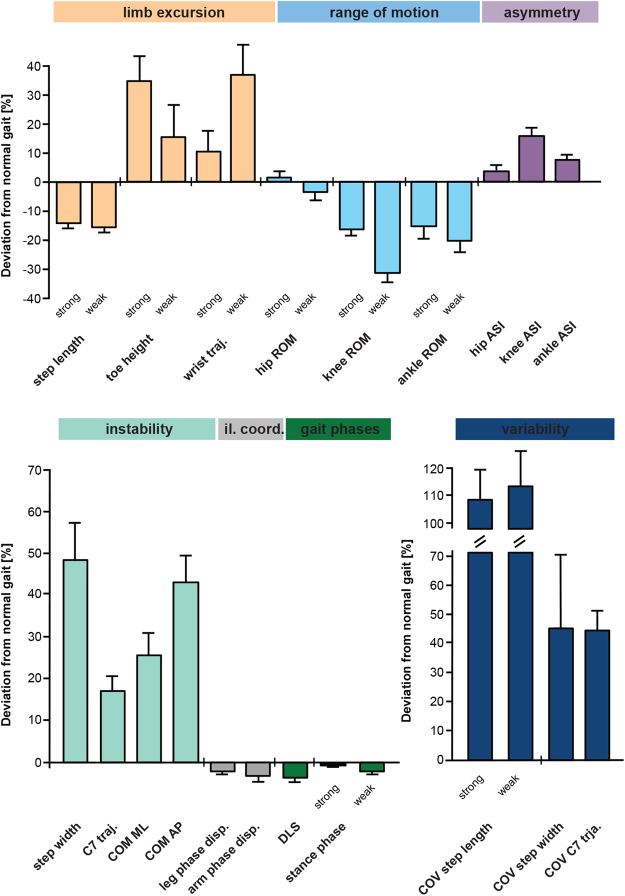
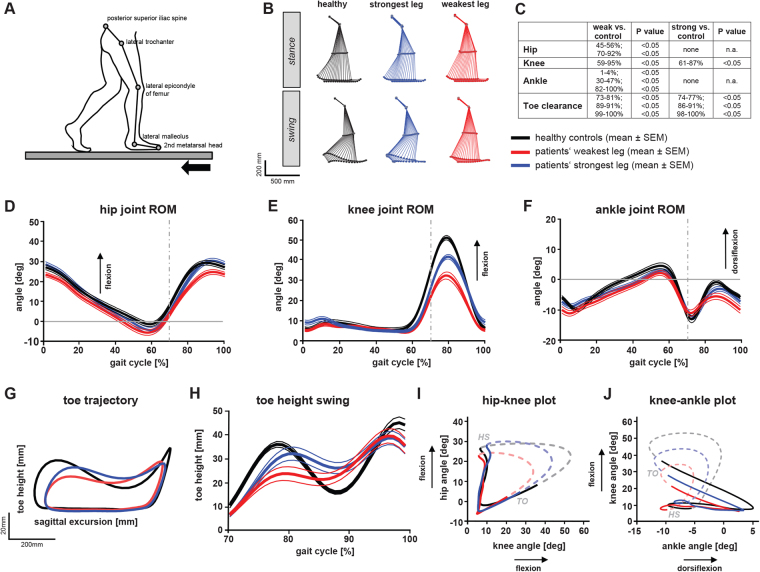
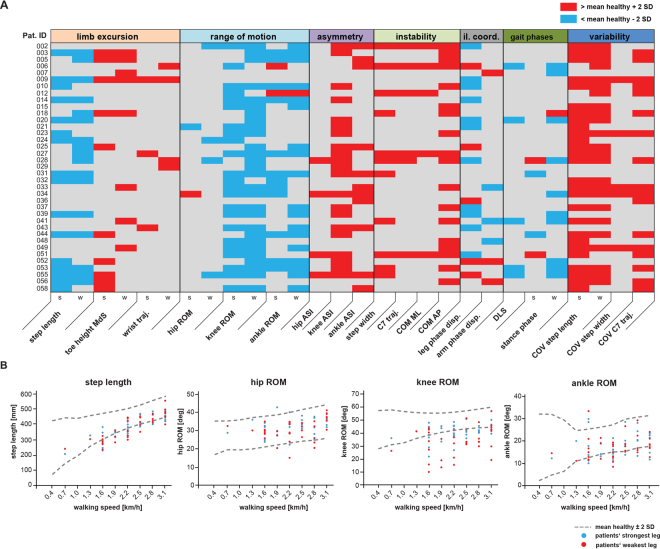
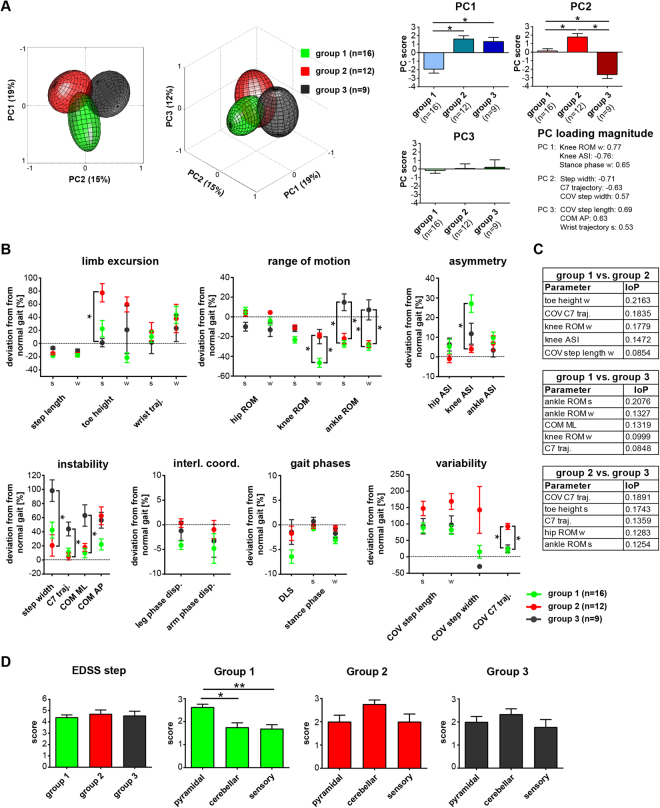
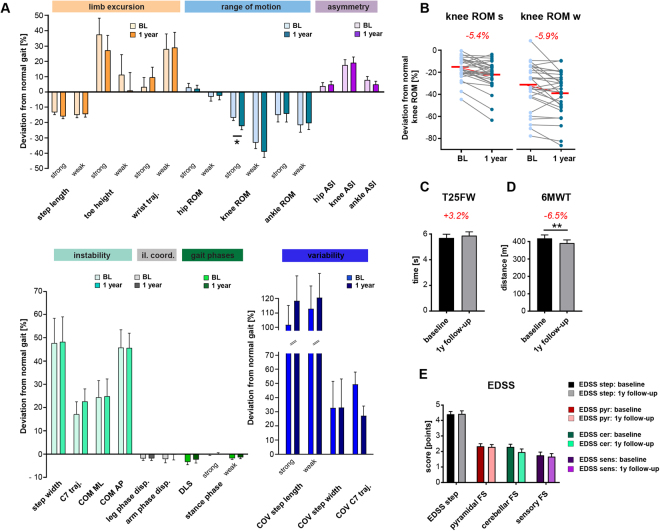
Gait dysfunction is a common and relevant symptom in multiple sclerosis (MS). This study aimed to profile gait pathology in gait-impaired patients with MS using comprehensive 3D gait analysis and clinical walking tests. Thirty-seven patients with MS walked on the treadmill at their individual, sustainable speed while 20 healthy control subjects walked at all the different patient's paces, allowing for comparisons independent of walking velocity. Kinematic analysis revealed pronounced restrictions in knee and ankle joint excursion, increased gait variability and asymmetry along with impaired dynamic stability in patients. The most discriminative single gait parameter, differentiating patients from controls with an accuracy of 83.3% (χ2 test; p = 0.0001), was reduced knee range of motion. Based on hierarchical cluster and principal component analysis, three principal pathological gait patterns were identified: a spastic-paretic, an ataxia-like, and an unstable gait. Follow-up assessments after 1 year indicated deterioration of walking function, particularly in patients with spastic-paretic gait patterns. Our findings suggest that impaired knee/ankle control is common in patients with MS. Personalised gait profiles and clustering algorithms may be promising tools for stratifying patients and to inform patient-tailored exercise programs. Responsive, objective outcome measures are important for monitoring disease progression and treatment effects in MS trials.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Scheinberg L, et al. Multiple sclerosis; earning a living. N Y State J Med. 1980;80:1395–1400. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
