

Addition of lactic acid levels improves the accuracy of quick sequential organ failure assessment in predicting mortality in surgical patients with complicated intra-abdominal infections: a retrospective study
- PMID: 29563963
- PMCID: PMC5851244
- DOI: 10.1186/s13017-018-0173-6
Addition of lactic acid levels improves the accuracy of quick sequential organ failure assessment in predicting mortality in surgical patients with complicated intra-abdominal infections: a retrospective study
Abstract
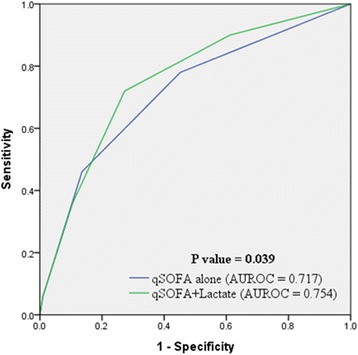
Background: The quick sequential organ failure assessment (qSOFA) alone has a poor sensitivity for predicting mortality in patients with complicated intra-abdominal infections, and plasma lactate levels have been shown to have a strong association with mortality in critically ill patients. Therefore, this study aimed to compare the performance of qSOFA with a score derived from a combination of qSOFA and serum lactate levels for predicting mortality in surgical patients with complicated intra-abdominal infections.
Methods: This retrospective study was performed at a university hospital. The medical records of 457 patients who presented to the emergency department (ED) between January 2008 and December 2016 and required emergency gastrointestinal surgery for a complicated intra-abdominal infection were reviewed retrospectively. qSOFA criteria, sequential organ failure assessment (SOFA) scores, and plasma lactate levels during their ED stay were collected. We performed area under receiver operating characteristic (AUROC) curve and sensitivity analysis to compare the performance of qSOFA alone with that of a score derived from the use of a combination of the qSOFA and lactate levels for predicting patient mortality.
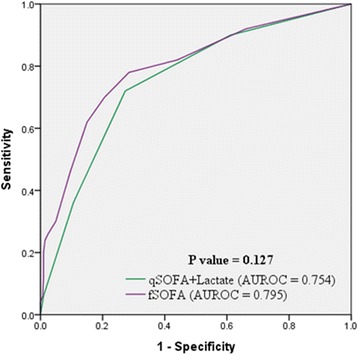
Results: Fifty patients (10.9%) died during hospitalization. The combined qSOFA and lactate level score was superior to qSOFA alone (AUROC = 0.754 vs. 0.717, p = 0.039, respectively) and comparable to the full SOFA score (AUROC = 0.754 vs. 0.795, p = 0.127, respectively) in predicting mortality. Sensitivity and specificity of qSOFA alone were 46 and 86%, respectively, and those of the combined score were 72 and 73%, respectively (p < 0.001).
Conclusion: A score derived from the qSOFA and serum lactate levels had better predictive performance with higher sensitivity than the qSOFA alone in predicting mortality in patients with complicated intra-abdominal infections and had a comparable predictive performance to that of the full SOFA score.
Keywords: Intra-abdominal infection; Lactate; Mortality; Retrospective studies.
Conflict of interest statement
This study was approved by the Institutional Review Board (4-2017-0726).Not applicableThe authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992;101:1644–1655. doi: 10.1378/chest.101.6.1644. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
