

Multivisceral resections for locally advanced colorectal cancer after preoperative treatment
- PMID: 29564129
- PMCID: PMC5854941
- DOI: 10.3892/mco.2018.1559
Multivisceral resections for locally advanced colorectal cancer after preoperative treatment
Abstract
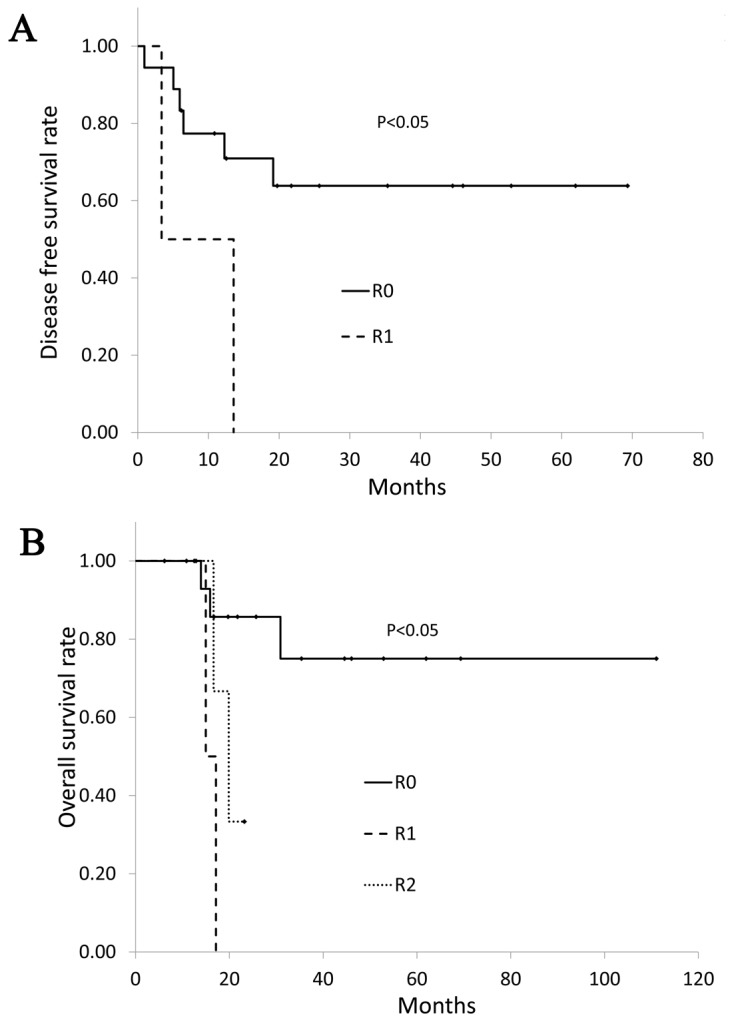
Multivisceral resection for colorectal cancer invading into the adjacent organs may often be difficult and may involve serious complications. Preoperative therapy may facilitate resection with safe margins. Between August 2007 and July 2016, 23 patients with colorectal cancer invading into the adjacent organs treated with preoperative treatment (chemoradiotherpay, chemotherapy, radiotherapy) were retrospectively investigated. All 23 patients received surgery with curative intent. Four patients had distant metastases at the time of diagnosis. Two patients had distant metastasis after preoperative treatment. The mean operative time was 535.3±185.5 min and the median amount of blood loss was 1,050 ml. Histopathological examination revealed malignant infiltration of the adjacent organs in 14 patients (60.9%). R0 resection rate was 73.9%. Postoperative complications were identified in nine patients (39.1%) and a high incidence of infectious complications was observed. Patients with curative resection showed a significantly better survival than patients with R1 or R2 resection (P<0.01). Multivisceral resection for locally advanced colorectal cancer invading into the adjacent organ after preoperative treatment may be performed with acceptable morbidity and minimal mortality. R0 resection improves the prognosis of patients with locally advanced colorectal cancer invading into the adjacent organ after preoperative treatment.
Keywords: chemoradiotherapy; chemotherapy; colorectal cancer; invasion; radiotherapy.
Figures
References
-
- Kashino I, Mizoue T, Tanaka K, Tsuji I, Tamakoshi A, Matsuo K, Wakai K, Nagata C, Inoue M, Tsugane S, et al. Research Group for Development and Evaluation of Cancer Prevention Strategies in Japan: Vegetable consumption and colorectal cancer risk: An evaluation based on a systematic review and meta-analysis among the Japanese population. Jpn J Clin Oncol. 2015;45:973–979. doi: 10.1093/jjco/hyv111. - DOI - PubMed
-
- Sobin LH, Gospodarowicz MK, Wittekind Ch. TMN classification of malignant tumours. 7th. Wiley-lckwell; Chichester, UK: 2010. UICC international union against cancer.
-
- Sugihara K. Japanese Society for Cancer of the Colon and Rectum, eds. Japanese Classification of Colorectal Carcinoma. 1st. Tokyo, Japan: Kanehara & Co Ltd; 1997. Response assessment of nonsurgical treatment for colorectal carcinoma; pp. 77–82.
LinkOut - more resources
Full Text Sources
Other Literature Sources