

Comparison of perioperative chemotherapy with adjuvant chemoradiotherapy for resectable gastric cancer: findings from a population-based study
- PMID: 29564169
- PMCID: PMC5848040
- DOI: 10.21037/jgo.2017.10.13
Comparison of perioperative chemotherapy with adjuvant chemoradiotherapy for resectable gastric cancer: findings from a population-based study
Abstract
Background: Both perioperative chemotherapy (PC) and adjuvant chemoradiotherapy (CRT) improve survival in resectable gastric cancer; however, these treatments have never been formally compared. Our objective was to evaluate treatment trends and compare survival outcomes for gastric cancer patients treated with surgery and either PC or CRT.
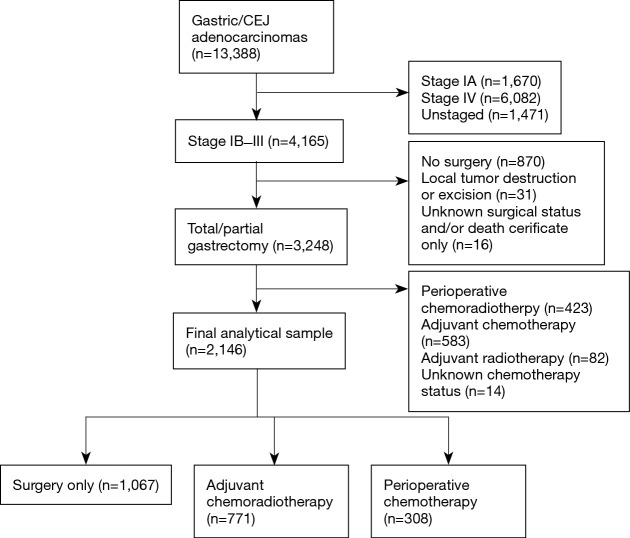
Methods: We performed a retrospective population-based cohort study between 2007 through 2013 using California Cancer Registry data. Patients diagnosed with stage IB-III gastric adenocarcinoma and treated with total or partial gastrectomy were eligible for this study. Based on the type of treatment received, patients were grouped into surgery-only, PC, or CRT. Primary and secondary outcomes were overall survival (OS) and gastric cancer-specific survival (GCCS) respectively. Mortality hazards ratios (HRs) for each of these outcomes were computed using propensity score weighted and covariate-adjusted Cox regression models, stratified by clinical node status.
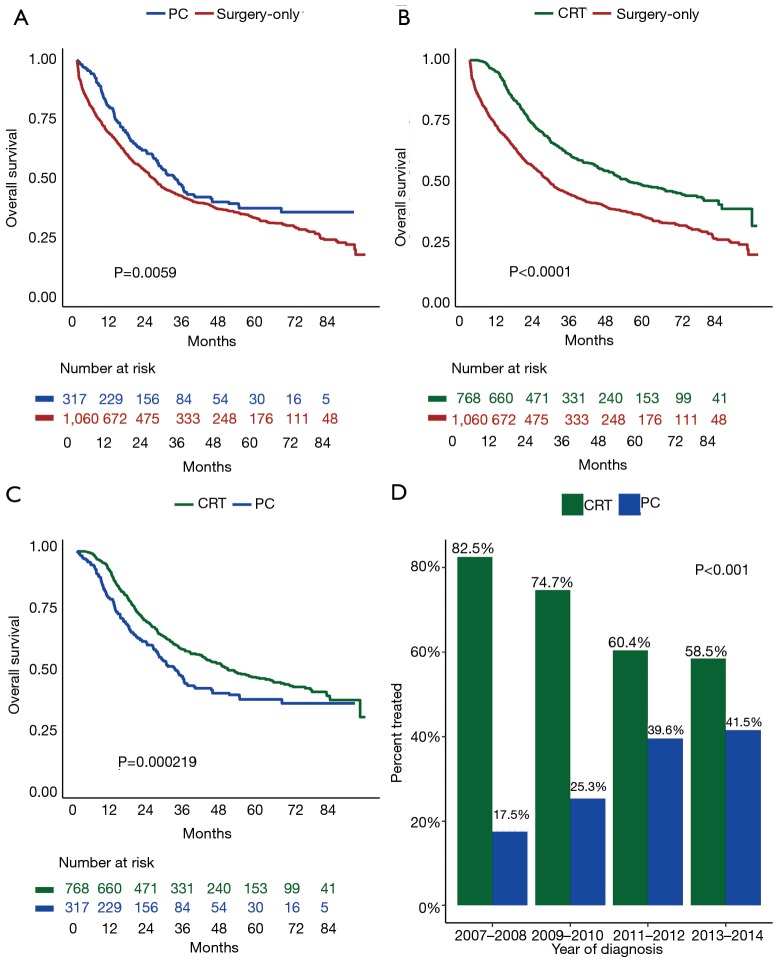
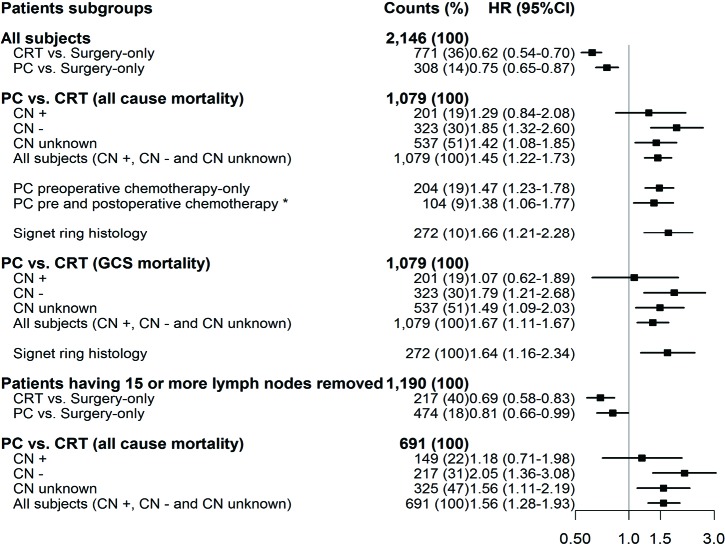
Results: Of 2,146 patients who underwent surgical resection, 1,067 had surgery-only, while 771 and 308 received PC or CRT, respectively. Median OS was 25, 33, and 52 months for surgery-only, PC, and CRT, respectively; P<0.001. Overall, patients treated with PC had significantly poorer survival compared to CRT (HR =1.45; 95% CI: 1.22-1.73). PC was also associated with higher mortality in patients with signet ring histology (HR =1.66; 95% CI: 1.21-2.28) and clinical node negative cancer (HR =1.85; 95% CI: 1.32-2.60). Survival was not different between PC vs. CRT in clinical node positive patients (HR =1.29; 95% CI: 0.84-2.08). Of note, the percentage of patients receiving PC increased from 17.5% in 2007-2008, to 41.5% in 2013-2014; P<0.001.
Conclusions: Despite the rapid adoption of PC, overall, CRT is associated with better survival than PC. Specifically, clinical node negative and signet ring histology patients had better survival when treated with CRT compared to PC. Based on these findings, we recommend against indiscriminate adoption of PC and consideration for CRT over PC in clinical node negative patients.
Keywords: Gastric cancer; adjuvant chemoradiotherapy (CRT); perioperative chemotherapy (PC).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Role of lymph node ratio in selection of adjuvant treatment (chemotherapy vs. chemoradiation) in patients with resected gastric cancer.J Gastrointest Oncol. 2018 Aug;9(4):708-717. doi: 10.21037/jgo.2018.05.12. J Gastrointest Oncol. 2018. PMID: 30151267 Free PMC article.
-
Lack of National Adoption of Evidence-Based Treatment for Resectable Gastric Adenocarcinoma.J Gastrointest Surg. 2021 Jan;25(1):36-47. doi: 10.1007/s11605-020-04868-0. Epub 2020 Nov 17. J Gastrointest Surg. 2021. PMID: 33201456 Free PMC article.
-
Implications of Lymph Node Staging on Selection of Adjuvant Therapy for Gastric Cancer in the United States: A Propensity Score-matched Analysis.Ann Surg. 2016 Feb;263(2):298-305. doi: 10.1097/SLA.0000000000001360. Ann Surg. 2016. PMID: 26135687
-
Effect of Chemoradiotherapy on the Survival of Resectable Gastric Cancer Patients: A Systematic Review and Meta-Analysis.Ann Surg Oncol. 2022 Oct;29(11):6962-6975. doi: 10.1245/s10434-022-12005-1. Epub 2022 Jun 20. Ann Surg Oncol. 2022. PMID: 35723792
-
Can adjuvant chemoradiotherapy replace extended lymph node dissection in gastric cancer?Recent Results Cancer Res. 2012;196:229-40. doi: 10.1007/978-3-642-31629-6_16. Recent Results Cancer Res. 2012. PMID: 23129378 Review.
Cited by
-
5-FU blocks shuttling of HuR mediated by PKCδ in gastric cancer cells.Transl Cancer Res. 2020 Aug;9(8):4790-4799. doi: 10.21037/tcr-20-2129. Transl Cancer Res. 2020. PMID: 35117842 Free PMC article.
-
Indications for adjuvant chemotherapy in patients with pT1N1M0 gastric cancer: a single-center experience.J Cancer Res Clin Oncol. 2021 Feb;147(2):561-568. doi: 10.1007/s00432-020-03355-y. Epub 2020 Aug 9. J Cancer Res Clin Oncol. 2021. PMID: 32772233 Free PMC article.
-
Comparison of Perioperative Chemotherapy versus Postoperative Chemoradiotherapy for Operable Stomach Cancer: A Western Canadian Province Experience.Curr Oncol. 2021 Mar 17;28(2):1262-1273. doi: 10.3390/curroncol28020120. Curr Oncol. 2021. PMID: 33802661 Free PMC article.
-
Quality of Life After Curative Resection for Gastric Cancer: Survey Metrics and Implications of Surgical Technique.J Surg Res. 2020 Jul;251:168-179. doi: 10.1016/j.jss.2020.02.005. Epub 2020 Mar 7. J Surg Res. 2020. PMID: 32151826 Free PMC article. Review.
-
Longitudinal Analysis of Quality-of-Life Recovery After Gastrectomy for Cancer.Ann Surg Oncol. 2021 Jan;28(1):48-56. doi: 10.1245/s10434-020-09274-z. Epub 2020 Oct 30. Ann Surg Oncol. 2021. PMID: 33125569 Free PMC article.
References
-
- Howlader N NA, Krapcho M, Garshell J, et al. editors. SEER Cancer Statistics Review. Bethesda, MD: National Cancer Institute, 1975-2013.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials