

Most Breast Cancer Patients with T1-2 Tumors and One to Three Positive Lymph Nodes Do Not Need Postmastectomy Radiotherapy
- PMID: 29564588
- PMCID: PMC5976529
- DOI: 10.1245/s10434-018-6422-9
Most Breast Cancer Patients with T1-2 Tumors and One to Three Positive Lymph Nodes Do Not Need Postmastectomy Radiotherapy
Abstract
Background/objective: Guidelines concur that postmastectomy radiation therapy (PMRT) in T1-2 tumors with one to three positive (+) lymph nodes (LNs) decreases locoregional recurrence (LRR) but advise limiting PMRT to patients at highest risk to balance against potential harms. In this study, we identify the risks of LRR after mastectomy in patients with T1-2N1 disease, treated with modern chemotherapy, and identify predictors of LRR when omitting PMRT.
Methods: Patients with T1-2N1 breast cancer undergoing mastectomy between 1995 and 2006 were categorized by receipt of PMRT. The Chi square test compared the clinicopathologic features between both groups, and Kaplan-Meier and Cox regression analysis was used to determine the rates of LRR, recurrence-free survival (RFS), and overall survival (OS).
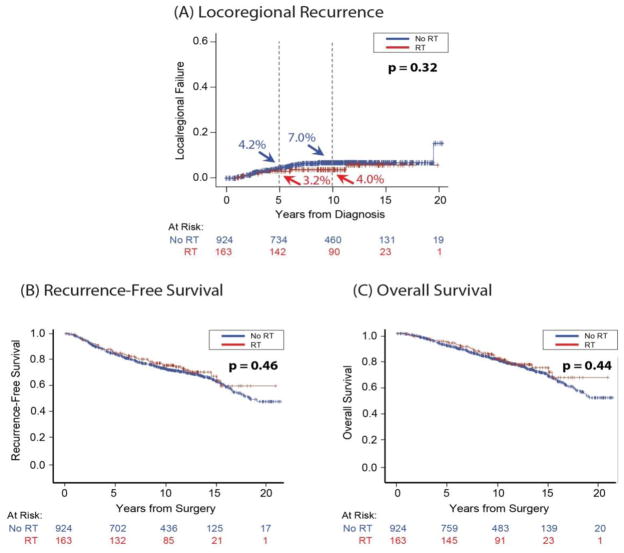
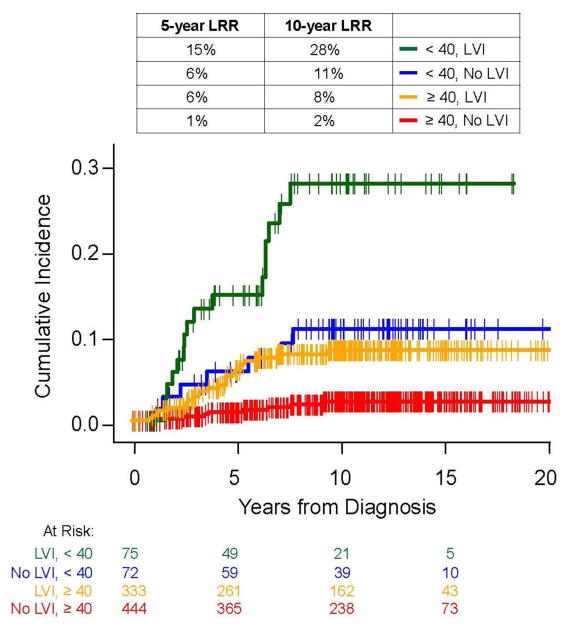
Results: Overall, 1087 patients (924 no PMRT, 163 PMRT) were included in the study, with a median follow-up of 10.8 years (range 0-21). We identified 63 LRRs (56 no PMRT, 7 PMRT), and 10-year rates of LRR with and without PMRT were 4.0% and 7.0%, respectively. Patients receiving PMRT were younger (p = 0.019), had larger tumors (p = 0.0013), higher histologic grade (p = 0.029), more positive LNs (p < 0.0001), lymphovascular invasion (LVI) (p < 0.0001), extracapsular nodal extension (p < 0.0001), and macroscopic LN metastases (p < 0.0001). There was no difference in LRR, RFS, or OS between groups. On multivariate analysis, age < 40 years (p < 0.0001) and LVI (p < 0.0001) were associated with LRR in those not receiving PMRT.
Conclusion: Consistent with the guidelines, 85% of patients with T1-2N1 were spared PMRT at our center, while maintaining low LRR. Age < 40 years and the presence of LVI are significantly associated with LRR in those not receiving PMRT.
Conflict of interest statement
Figures
Comment in
-
ASO Author Reflections: Locoregional Recurrence Rates are Low with the Selective Use of PMRT in Patients with T1-2 Tumors and One to Three Positive Lymph Nodes.Ann Surg Oncol. 2018 Dec;25(Suppl 3):691-692. doi: 10.1245/s10434-018-7010-8. Epub 2018 Nov 21. Ann Surg Oncol. 2018. PMID: 30465226 Free PMC article. No abstract available.
Similar articles
-
Selection criteria for postmastectomy radiotherapy in t1-t2 tumors with 1 to 3 positive lymph nodes.Ann Surg Oncol. 2013 Oct;20(10):3169-74. doi: 10.1245/s10434-013-3117-0. Epub 2013 Aug 22. Ann Surg Oncol. 2013. PMID: 23975289
-
Minimal impact of postmastectomy radiation therapy on locoregional recurrence for breast cancer patients with 1 to 3 positive lymph nodes in the modern treatment era.Surg Oncol. 2017 Jun;26(2):163-170. doi: 10.1016/j.suronc.2017.03.003. Epub 2017 Mar 16. Surg Oncol. 2017. PMID: 28577722
-
Impact of molecular subtype on locoregional recurrence in mastectomy patients with T1-T2 breast cancer and 1-3 positive lymph nodes.Ann Surg Oncol. 2014 May;21(5):1569-74. doi: 10.1245/s10434-014-3488-x. Epub 2014 Feb 1. Ann Surg Oncol. 2014. PMID: 24488216 Free PMC article.
-
Postmastectomy radiation therapy in early breast cancer: Utility or futility?Crit Rev Oncol Hematol. 2020 Mar;147:102887. doi: 10.1016/j.critrevonc.2020.102887. Epub 2020 Jan 30. Crit Rev Oncol Hematol. 2020. PMID: 32018127 Review.
-
Post-mastectomy radiation therapy in breast cancer patients with 1-3 positive lymph nodes: No one size fits all.Crit Rev Oncol Hematol. 2020 Mar;147:102880. doi: 10.1016/j.critrevonc.2020.102880. Epub 2020 Jan 18. Crit Rev Oncol Hematol. 2020. PMID: 32045847 Review.
Cited by
-
Breast Cancer: An Overview of Current Therapeutic Strategies, Challenge, and Perspectives.Breast Cancer (Dove Med Press). 2023 Oct 20;15:721-730. doi: 10.2147/BCTT.S432526. eCollection 2023. Breast Cancer (Dove Med Press). 2023. PMID: 37881514 Free PMC article. Review.
-
A multi-institutional prediction model to estimate the risk of recurrence and mortality after mastectomy for T1-2N1 breast cancer.Cancer. 2022 Aug 15;128(16):3057-3066. doi: 10.1002/cncr.34352. Epub 2022 Jun 17. Cancer. 2022. PMID: 35713598 Free PMC article.
-
Development and validation of nomograms for predicting survival outcomes in patients with T1-2N1 breast cancer to identify those who could not benefit from postmastectomy radiotherapy.Front Oncol. 2023 Mar 28;13:1112687. doi: 10.3389/fonc.2023.1112687. eCollection 2023. Front Oncol. 2023. PMID: 37056328 Free PMC article.
-
RecurIndex-Guided postoperative radiotherapy with or without Avoidance of Irradiation of regional Nodes in 1-3 node-positive breast cancer (RIGAIN): a study protocol for a multicentre, open-label, randomised controlled prospective, phase III trial.BMJ Open. 2024 Jul 30;14(7):e078049. doi: 10.1136/bmjopen-2023-078049. BMJ Open. 2024. PMID: 39079921 Free PMC article.
-
The significance of risk stratification through nomogram-based assessment in determining postmastectomy radiotherapy for patients diagnosed with pT1 - 2N1M0 breast cancer.Radiat Oncol. 2024 Sep 13;19(1):120. doi: 10.1186/s13014-024-02510-w. Radiat Oncol. 2024. PMID: 39272162 Free PMC article.
References
-
- Early Breast Cancer Trialists' Collaborative Group (EBCTCG) McGale P, Taylor C, Correa C, Cutter D, Duane F, Ewertz M, et al. Effect of radiotherapy after mastectomy and axillary surgery on 10-year recurrence and 20-year breast cancer mortality: meta-analysis of individual patient data for 8135 women in 22 randomised trials. Lancet. 2014;383(9935):2127–35. - PMC - PubMed
-
- Clarke M, Collins R, Darby S, Davies C, Elphinstone P, Evans V, Godwin J, et al. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;366(9503):2087–106. - PubMed
-
- The National Institutes of Health Consensus Development Conference: Adjuvant Therapy for Breast Cancer. Bethesda, Maryland, USA. November 1–3, 2000. Proceedings. J Natl Cancer Inst Monogr. 2001;(30):1–152. - PubMed
-
- Killander F, Anderson H, Ryden S, Moller T, Aspegren K, Ceberg J, Danewid C, et al. Radiotherapy and tamoxifen after mastectomy in postmenopausal women -- 20 year follow-up of the South Sweden Breast Cancer Group randomised trial SSBCG II:I. Eur J Cancer. 2007;43(14):2100–8. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
