

The Postprandial-to-Fasting Serum C-Peptide Ratio is a Predictor of Response to Basal Insulin-Supported Oral Antidiabetic Drug(s) Therapy: A Retrospective Analysis
- PMID: 29564716
- PMCID: PMC5984910
- DOI: 10.1007/s13300-018-0404-6
The Postprandial-to-Fasting Serum C-Peptide Ratio is a Predictor of Response to Basal Insulin-Supported Oral Antidiabetic Drug(s) Therapy: A Retrospective Analysis
Abstract
Introduction: Basal insulin is widely recommended for the treatment of type 2 diabetes mellitus (T2DM) patients who are unable to achieve glycemic control with oral antidiabetic drug(s) (OADs). However, some patients are still unable to control their blood glucose levels even when on basal insulin-supported OAD(s) therapy (BOT). The aim of this study was to investigate the factor(s) predicting patient response to BOT.
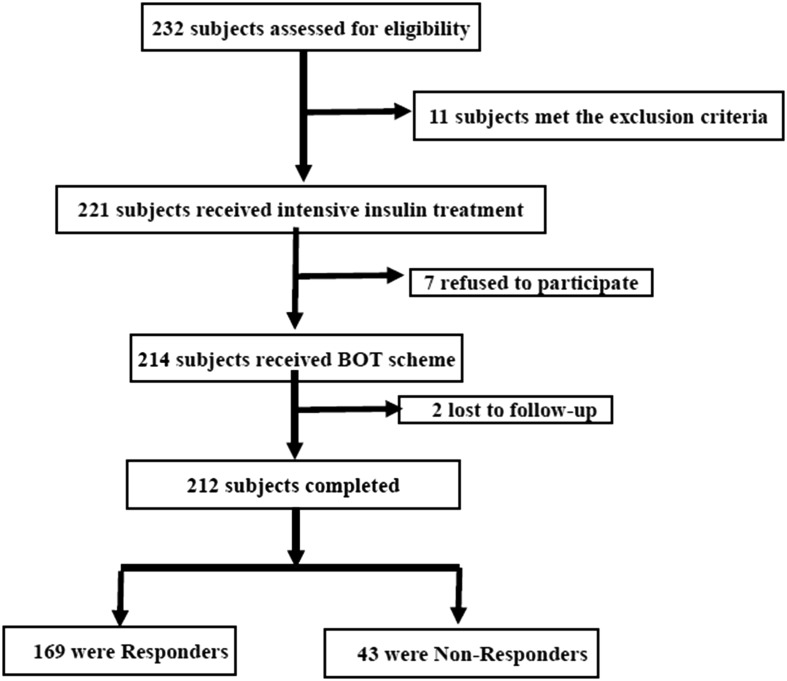
Methods: A total of 212 patients with T2DM, ranging in age from 18 to 65 years, admitted to the university hospital of Sun Yat-sen University, Guangzhou, China, were enrolled in the study between January 2013 and July 2016. All patients had fasting blood glucose levels of ≥ 10.0 mmol/L despite receiving OAD(s) treatment. According to study design, these patients first received intensive insulin therapy for 2 weeks to attain and maintain their glycemic goals and then were switched to BOT. Responders were defined as subjects who maintained their glycemic targets with BOT for at least 3 months; all others were considered to be non-responders. The characteristics between responders and non-responders were compared.
Results: Compared with non-responders, responders had a shorter duration of diabetes (5.1 ± 5.0 vs. and 10.1 ± 3.2 years; P < 0.001) and a higher 2-h postprandial C-peptide-to-fasting C-peptide ratio (2 h-PCP/FCP: 1.95 ± 0.51 vs. 1.67 ± 0.32; P < 0.01). Responders showed a lower proportion of previous treatment with insulin (69/100 vs 40/3; P < 0.001) and sulfonlureas or glinides (116/50 vs 40/0; P <0.001) than non-responders. Multivariate logistic regression analysis showed that previous insulin treatment (odds ratio [OR] 17.677, 95% confidence interval [CI] 5.205-60.027; P < 0.001) and the 2 h-PCP/FCP ratio (OR 0.241, 95% CI 0.058-0.679; P = 0.007) had predictive value.
Conclusions: A higher 2 h-PCP/FCP ratio and a lack of previous insulin treatment increase the likelihood of BOT success.
Keywords: Basal insulin; C-peptide; Predictor; Type 2 diabetes mellitus.
Figures
Similar articles
-
Treatment intensification using long-acting insulin -predictors of future basal insulin supported oral therapy in the DIVE registry.BMC Endocr Disord. 2015 Oct 7;15:54. doi: 10.1186/s12902-015-0051-0. BMC Endocr Disord. 2015. PMID: 26446863 Free PMC article.
-
Association between the preoperative fasting and postprandial C-peptide AUC with resolution of type 2 diabetes 6 months following bariatric surgery.Metabolism. 2015 Nov;64(11):1556-63. doi: 10.1016/j.metabol.2015.08.009. Epub 2015 Aug 18. Metabolism. 2015. PMID: 26386694
-
EADSG Guidelines: Insulin Therapy in Diabetes.Diabetes Ther. 2018 Apr;9(2):449-492. doi: 10.1007/s13300-018-0384-6. Epub 2018 Mar 5. Diabetes Ther. 2018. PMID: 29508275 Free PMC article.
-
Advancing therapy in type 2 diabetes mellitus with early, comprehensive progression from oral agents to insulin therapy.Clin Ther. 2007;29 Spec No:1236-53. Clin Ther. 2007. PMID: 18046925 Review.
-
Repaglinide : a pharmacoeconomic review of its use in type 2 diabetes mellitus.Pharmacoeconomics. 2004;22(6):389-411. doi: 10.2165/00019053-200422060-00005. Pharmacoeconomics. 2004. PMID: 15099124 Review.
Cited by
-
Predictive value of postprandial C-peptide for utilizing multiple daily injection therapy in type 2 diabetes.Endocrine. 2024 Sep;85(3):1162-1169. doi: 10.1007/s12020-024-03820-5. Epub 2024 Apr 15. Endocrine. 2024. PMID: 38622435
-
The efficacy of switching basal-bolus insulin therapy to basal insulin-supported oral therapy with a glinide and an α-glucosidase inhibitor in patients with type 2 diabetes depends on insulin secretory capacity, but not on blood glucose profiles and insulin dosages prior to the switching.Diabetol Int. 2023 Sep 4;15(1):99-108. doi: 10.1007/s13340-023-00651-z. eCollection 2024 Jan. Diabetol Int. 2023. PMID: 38264217 Free PMC article.
References
-
- Nathan DM, Buse JB, Davidson MB, Ferrannini E, Holman RR, Sherwin R, et al. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2009;32:193–203. doi: 10.2337/dc08-9025. - DOI - PMC - PubMed
Grants and funding
- 2015015/5010 Clinical Research Projects of Sun Yat-sen University
- 2016A050502010/the Science and Technology Plan Projects of Guangdong Province
- 201604020016/the Key Special Projects of Medical and Health Collaborative Innovation of Guangzhou City
- 2060404/the Special Scientific Research Project of Guangzhou City
- 2017YFA0105803/National Key R&D Program of China
LinkOut - more resources
Full Text Sources
Other Literature Sources
