

Potentially modifiable respiratory variables contributing to outcome in ICU patients without ARDS: a secondary analysis of PRoVENT
- PMID: 29564726
- PMCID: PMC5862714
- DOI: 10.1186/s13613-018-0385-7
Potentially modifiable respiratory variables contributing to outcome in ICU patients without ARDS: a secondary analysis of PRoVENT
Abstract
Background: The majority of critically ill patients do not suffer from acute respiratory distress syndrome (ARDS). To improve the treatment of these patients, we aimed to identify potentially modifiable factors associated with outcome of these patients.
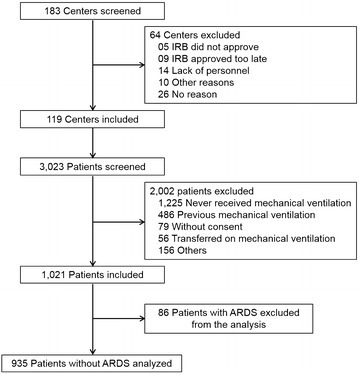
Methods: The PRoVENT was an international, multicenter, prospective cohort study of consecutive patients under invasive mechanical ventilatory support. A predefined secondary analysis was to examine factors associated with mortality. The primary endpoint was all-cause in-hospital mortality.
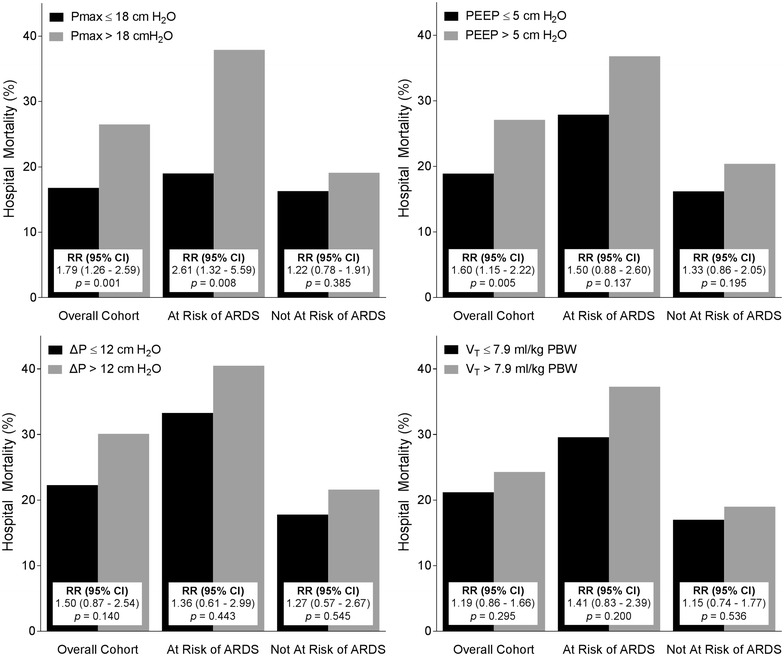
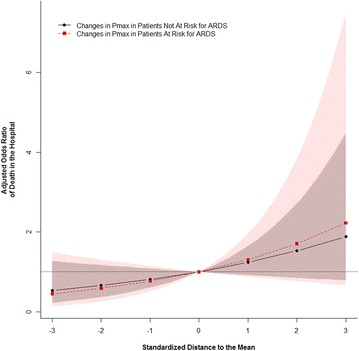
Results: 935 Patients were included. In-hospital mortality was 21%. Compared to patients who died, patients who survived had a lower risk of ARDS according to the 'Lung Injury Prediction Score' and received lower maximum airway pressure (Pmax), driving pressure (ΔP), positive end-expiratory pressure, and FiO2 levels. Tidal volume size was similar between the groups. Higher Pmax was a potentially modifiable ventilatory variable associated with in-hospital mortality in multivariable analyses. ΔP was not independently associated with in-hospital mortality, but reliable values for ΔP were available for 343 patients only. Non-modifiable factors associated with in-hospital mortality were older age, presence of immunosuppression, higher non-pulmonary sequential organ failure assessment scores, lower pulse oximetry readings, higher heart rates, and functional dependence.
Conclusions: Higher Pmax was independently associated with higher in-hospital mortality in mechanically ventilated critically ill patients under mechanical ventilatory support for reasons other than ARDS. Trial Registration ClinicalTrials.gov (NCT01868321).
Keywords: Mechanical ventilation; Mortality; Outcome; Ventilator settings.
Figures
References
-
- Serpa Neto A, Simonis FD, Barbas CSV, et al. Association between tidal volume size, duration of ventilation, and sedation needs in patients without acute respiratory distress syndrome: an individual patient data meta-analysis. Intensive Care Med. 2014;40:950–957. doi: 10.1007/s00134-014-3318-4. - DOI - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
