

On what basis are medical cost-effectiveness thresholds set? Clashing opinions and an absence of data: a systematic review
- PMID: 29564962
- PMCID: PMC5930346
- DOI: 10.1080/16549716.2018.1447828
On what basis are medical cost-effectiveness thresholds set? Clashing opinions and an absence of data: a systematic review
Abstract
Background: The amount a government should be willing to invest in adopting new medical treatments has long been under debate. With many countries using formal cost-effectiveness (C/E) thresholds when examining potential new treatments and ever-growing medical costs, accurately setting the level of a C/E threshold can be essential for an efficient healthcare system.
Objectives: The aim of this systematic review is to describe the prominent approaches to setting a C/E threshold, compile available national-level C/E threshold data and willingness-to-pay (WTP) data, and to discern whether associations exist between these values, gross domestic product (GDP) and health-adjusted life expectancy (HALE). This review further examines current obstacles faced with the presently available data.
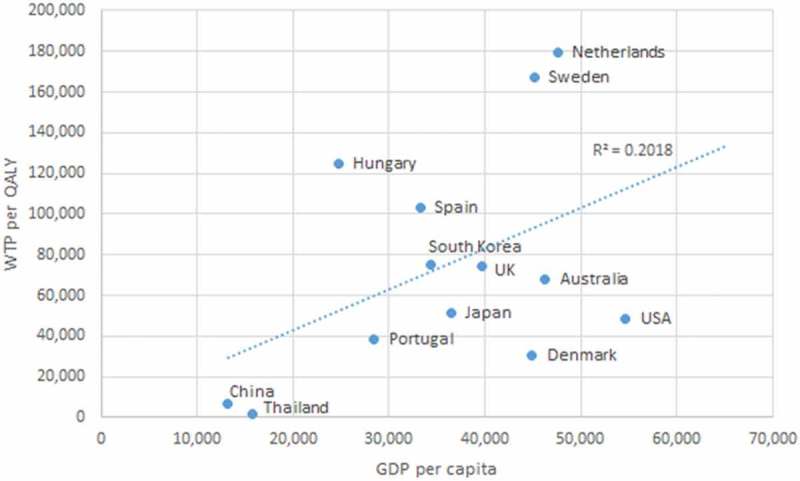
Methods: A systematic review was performed to collect articles which have studied national C/E thresholds and willingness-to-pay (WTP) per quality-adjusted life year (QALY) in the general population. Associations between GDP, HALE, WTP, and C/E thresholds were analyzed with correlations.
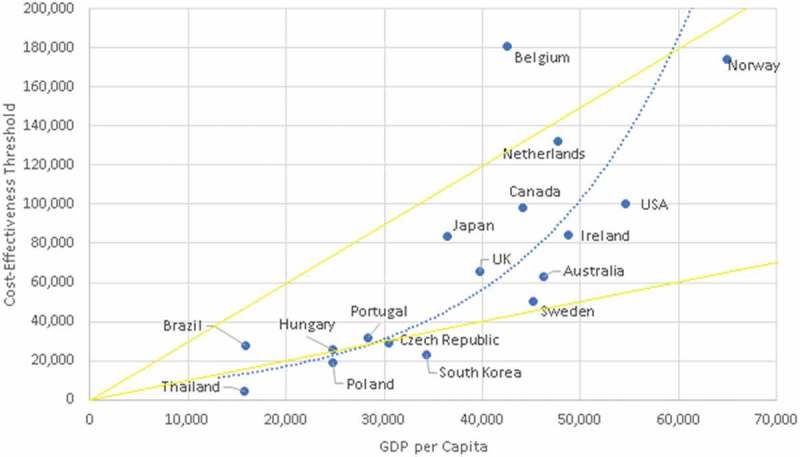
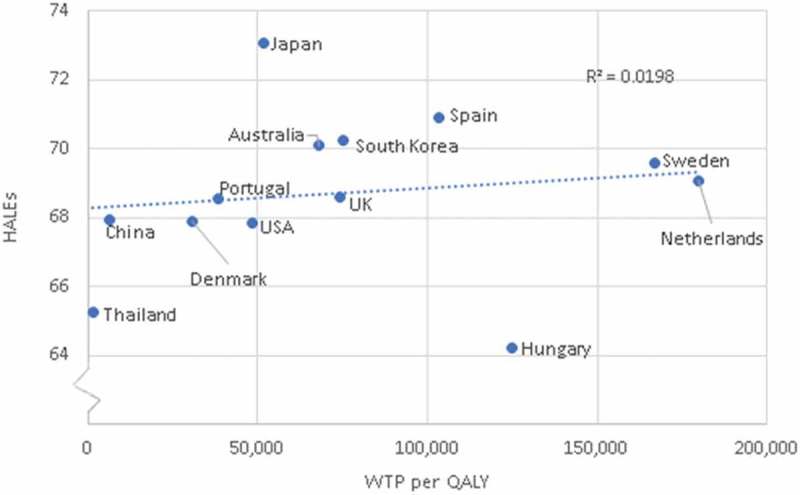
Results: Seventeen countries were identified from nine unique sources to have formal C/E thresholds within our inclusion criteria. Thirteen countries from nine sources were identified to have WTP per QALY data within our inclusion criteria. Two possible associations were identified: C/E thresholds with HALE (quadratic correlation of 0.63), and C/E thresholds with GDP per capita (polynomial correlation of 0.84). However, these results are based on few observations and therefore firm conclusions cannot be made.
Conclusions: Most national C/E thresholds identified in our review fall within the WHO's recommended range of one-to-three times GDP per capita. However, the quality and quantity of data available regarding national average WTP per QALY, opportunity costs, and C/E thresholds is poor in comparison to the importance of adequate investment in healthcare. There exists an obvious risk that countries might either over- or underinvest in healthcare if they base their decision-making process on erroneous presumptions or non-evidence-based methodologies. The commonly referred to value of 100,000$ USD per QALY may potentially have some basis.
Keywords: C/E thresholds; HALE; QALY; WTP; cost-effective; decision-making; healthy adjusted life expectancy; international; systematic review; willing-to-pay.
Conflict of interest statement
No potential conflict of interest was reported by the authors.
Figures





References
-
- Claxton K, Martin S, Soares M, et al. Systematic review of the literature on the cost-effectiveness threshold. 2015 [cited 2017 November2]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK274312/
-
- Cleemput I, Neyt M, Thiry N, et al. Using threshold values for cost per quality-adjusted life-year gained in healthcare decisions. Int J Technol Assess Health Care. 2011;27:71–14. - PubMed
-
- Schwarzer R, Rochau U, Saverno K, et al. Systematic overview of cost–effectiveness thresholds in ten countries across four continents. J Comp Eff Res. 2015;4:485–504. - PubMed
-
- Neumann PJ, Sandberg EA, Bell CM, et al. Are pharmaceuticals cost-effective? A review of the evidence. Health Aff. 2000;19:92–109. - PubMed
-
- Baker R, Chilton S, Donaldson C, et al. Searchers vs surveyors in estimating the monetary value of a QALY: resolving a nasty dilemma for NICE. Health Econ Policy Law. 2011;6:435–447. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical