

Impact of frailty on outcomes after discharge in older surgical patients: a prospective cohort study
- PMID: 29565018
- PMCID: PMC5828889
- DOI: 10.1503/cmaj.161403
Impact of frailty on outcomes after discharge in older surgical patients: a prospective cohort study
Abstract
Background: Frailty is a state of vulnerability to diverse stressors. We assessed the impact of frailty on outcomes after discharge in older surgical patients.
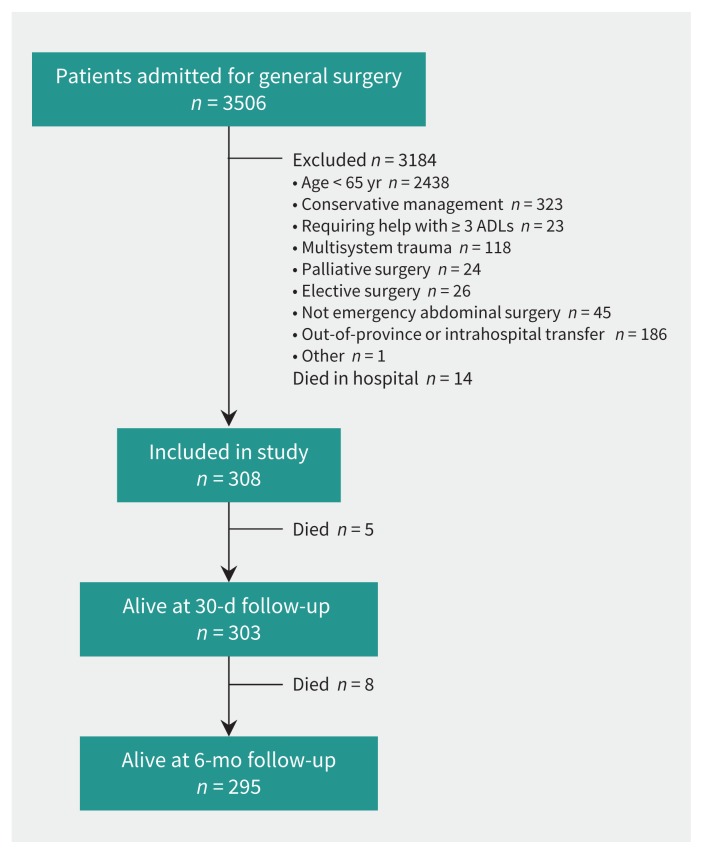
Methods: We prospectively followed patients 65 years of age or older who underwent emergency abdominal surgery at either of 2 tertiary care centres and who needed assistance with fewer than 3 activities of daily living. Preadmission frailty was defined according to the Canadian Study of Health and Aging Clinical Frailty Scale as "well" (score 1 or 2), "vulnerable" (score 3 or 4) or "frail" (score 5 or 6). We assessed composite end points of 30-day and 6-month all-cause readmission or death by multivariable logistic regression.
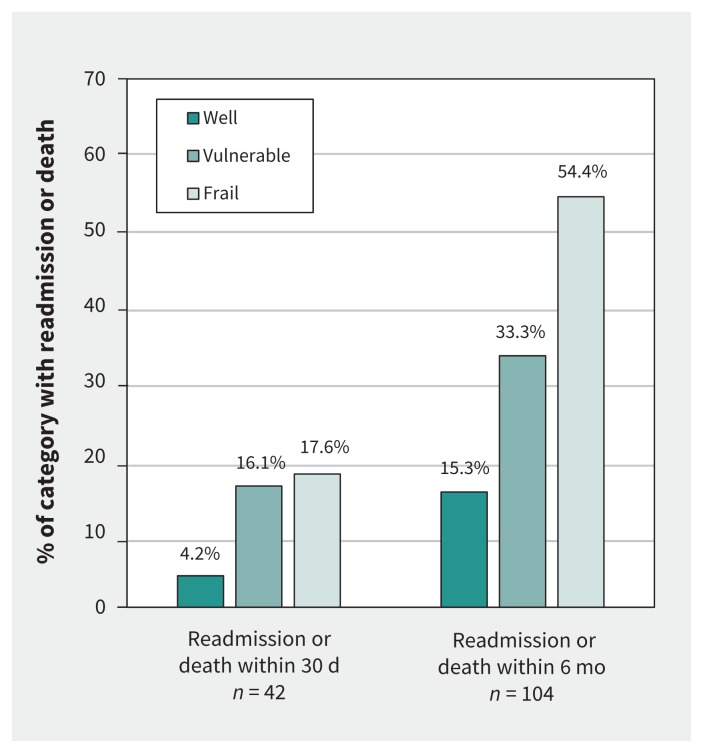
Results: Of 308 patients (median age 75 [range 65-94] yr, median Clinical Frailty Score 3 [range 1-6]), 168 (54.5%) were classified as vulnerable and 68 (22.1%) as frail. Ten (4.2%) of those classified as vulnerable or frail received a geriatric consultation. At 30 days after discharge, the proportions of patients who were readmitted or had died were greater among vulnerable patients (n = 27 [16.1%]; adjusted odds ratio [OR] 4.60, 95% confidence interval [CI] 1.29-16.45) and frail patients (n = 12 [17.6%]; adjusted OR 4.51, 95% CI 1.13-17.94) than among patients who were well (n = 3 [4.2%]). By 6 months, the degree of frailty independently and dose-dependently predicted readmission or death: 56 (33.3%) of the vulnerable patients (adjusted OR 2.15, 95% CI 1.01-4.55) and 37 (54.4%) of the frail patients (adjusted OR 3.27, 95% CI 1.32-8.12) were readmitted or had died, compared with 11 (15.3%) of the patients who were well.
Interpretation: Vulnerability and frailty were prevalent in older patients undergoing surgery and unlikely to trigger specialized geriatric assessment, yet remained independently associated with greater risk of readmission for as long as 6 months after discharge. Therefore, the degree of frailty has important prognostic value for readmission.
Trial registration for primary study: ClinicalTrials.gov, no. NCT02233153.
© 2018 Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Using frailty tools as prognostic markers in patients who are acutely ill.CMAJ. 2018 Feb 20;190(7):E182-E183. doi: 10.1503/cmaj.170902. CMAJ. 2018. PMID: 29565017 Free PMC article. No abstract available.
-
Discharge outcomes and frailty.CMAJ. 2019 Apr 8;191(14):E402. doi: 10.1503/cmaj.71600. CMAJ. 2019. PMID: 30962201 Free PMC article. No abstract available.
References
-
- All-cause readmission to acute care and return to the emergency department. Ottawa: Canadian Institute for Health Information; 2012.
-
- Readmissions reduction program (HRRP). Baltimore: Centers for Medicare & Medicaid Services; 2016. Available: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpat... (accessed 2016 Nov. 8).
-
- Population projections for Canada, provinces and territories: 2009 to 2036. Cat no 91-520-X. Ottawa: Statistics Canada; 2010. Available: www.statcan.gc.ca/pub/91-520-x/91-520-x2010001-eng.pdf (accessed 2016 Nov. 8).
-
- Holt PJE, Poloniecki JD, Hofman D, et al. Re-interventions, readmissions and discharge destination: modern metrics for the assessment of the quality of care. Eur J Vasc Endovasc Surg 2010;39:49–54. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical