

An unfavorable body composition is common in early arthritis patients: A case control study
- PMID: 29565986
- PMCID: PMC5863963
- DOI: 10.1371/journal.pone.0193377
An unfavorable body composition is common in early arthritis patients: A case control study
Abstract
Background: An unfavorable body composition is often present in chronic arthritis patients. This unfavorable composition is a loss of muscle mass, with a stable or increased (abdominal) fat mass. Since it is unknown when this unfavorable composition develops, we compared body composition in disease-modifying antirheumatic drugs (DMARD)-naive early arthritis patients with non-arthritis controls and explored the association, in early arthritis patients, with disease activity and traditional cardiovascular risk factors.
Methods: 317 consecutive early arthritis patients (84% rheumatoid arthritis according to 2010 ACR/EULAR criteria) and 1268 age-/gender-/ethnicity-matched non-arthritis controls underwent a Dual-energy X-ray absorptiometry scan to assess fat percentage, fat mass index, fat mass distribution and appendicular lean (muscle) mass index. Additionally, disease activity, health assessment questionnaire (HAQ), acute phase proteins, lipid profile and blood pressure were evaluated.
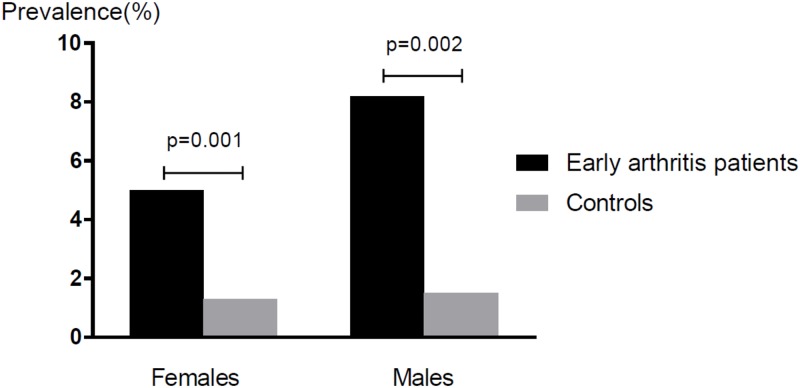
Results: Loss of muscle mass (corrected for age suspected muscle mass) was 4-5 times more common in early arthritis patients, with a significantly lower mean appendicular lean mass index (females 6% and males 7% lower, p<0.01). Patients had more fat distributed to the trunk (females p<0.01, males p = 0.07) and females had a 4% higher mean fat mass index (p<0.01). An unfavorable body composition was associated with a higher blood pressure and an atherogenic lipid profile. There was no relationship with disease activity, HAQ or acute phase proteins.
Conclusion: Loss of muscle mass is 4-5 times more common in early arthritis patients, and is in early arthritis patients associated with a higher blood pressure and an atherogenic lipid profile. Therefore, cardiovascular risk is already increased at the clinical onset of arthritis making cardiovascular risk management necessary in early arthritis patients.
Conflict of interest statement
Figures
References
-
- Braun J, Kruger K, Manger B, Schneider M, Specker C, Trappe HJ. Cardiovascular Comorbidity in Inflammatory Rheumatological Conditions. Dtsch Arztebl Int 2017;114:197–203. doi: 10.3238/arztebl.2017.0197 - DOI - PMC - PubMed
-
- Nurmohamed MT, Heslinga M, Kitas GD. Cardiovascular comorbidity in rheumatic diseases. Nat Rev Rheumatol 2015;11:693–704. doi: 10.1038/nrrheum.2015.112 - DOI - PubMed
-
- Holmqvist ME, Wedren S, Jacobsson LT, Klareskog L, Nyberg F, Rantapaa-Dahlqvist S, et al. Rapid increase in myocardial infarction risk following diagnosis of rheumatoid arthritis amongst patients diagnosed between 1995 and 2006. J Intern Med 2010;268:578–85. doi: 10.1111/j.1365-2796.2010.02260.x - DOI - PubMed
-
- Innala L, Moller B, Ljung L, Magnusson S, Smedby T, Sodergren A, et al. Cardiovascular events in early RA are a result of inflammatory burden and traditional risk factors: a five year prospective study. Arthritis Res Ther 2011;13:R131 doi: 10.1186/ar3442 - DOI - PMC - PubMed
-
- Kerola AM, Kauppi MJ, Kerola T, Nieminen TV. How early in the course of rheumatoid arthritis does the excess cardiovascular risk appear? Ann Rheum Dis 2012;71:1606–15. doi: 10.1136/annrheumdis-2012-201334 - DOI - PubMed
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
