

Low serum sodium levels at hospital admission: Outcomes among 2.3 million hospitalized patients
- PMID: 29566068
- PMCID: PMC5864034
- DOI: 10.1371/journal.pone.0194379
Low serum sodium levels at hospital admission: Outcomes among 2.3 million hospitalized patients
Abstract
Background: Hyponatremia is the most common electrolyte disorder among hospitalized patients. Controversies still exist over the relationship between hyponatremia and outcomes of hospitalized patients.
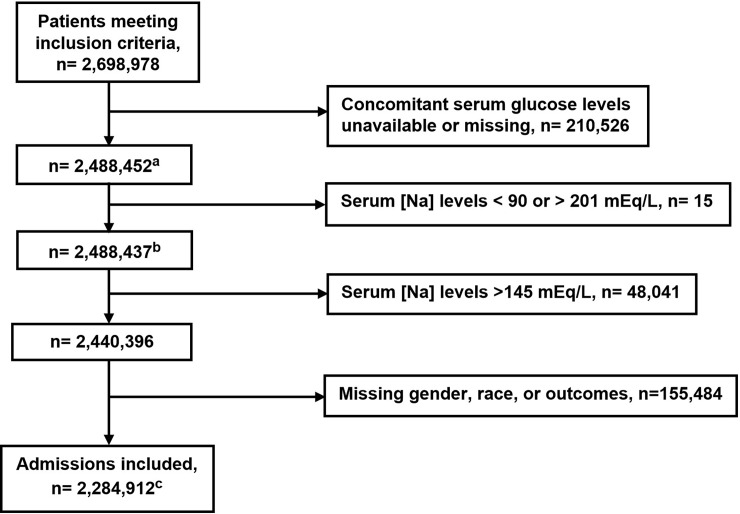
Methods: To analyze the association of low serum sodium levels at hospital admission with in-hospital mortality and patient disposition and to compare the distribution of the risk of death associated with hyponatremia across the lifespan of hospitalized patients, we conducted an observational study of 2.3 million patients using data extracted from the Cerner Health Facts database between 2000 and 2014. Logistic regression models were used in the analyses.
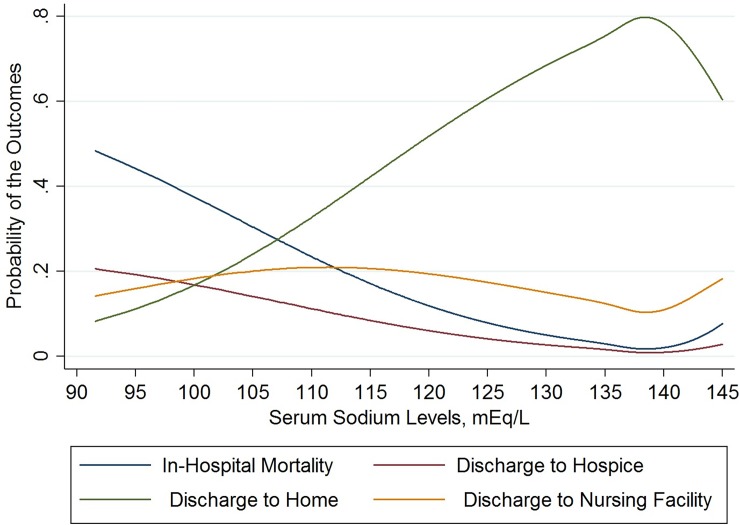
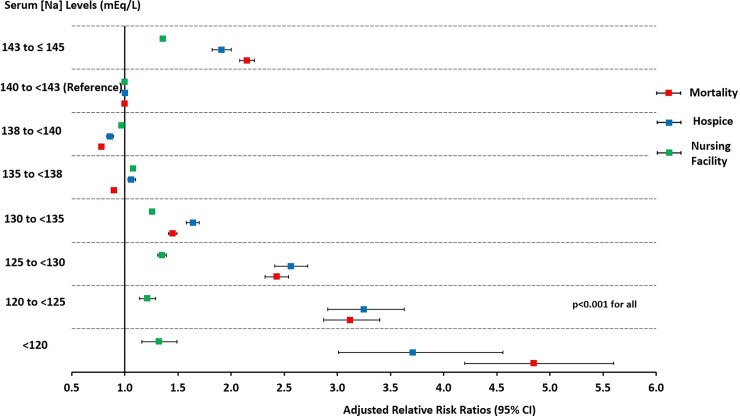
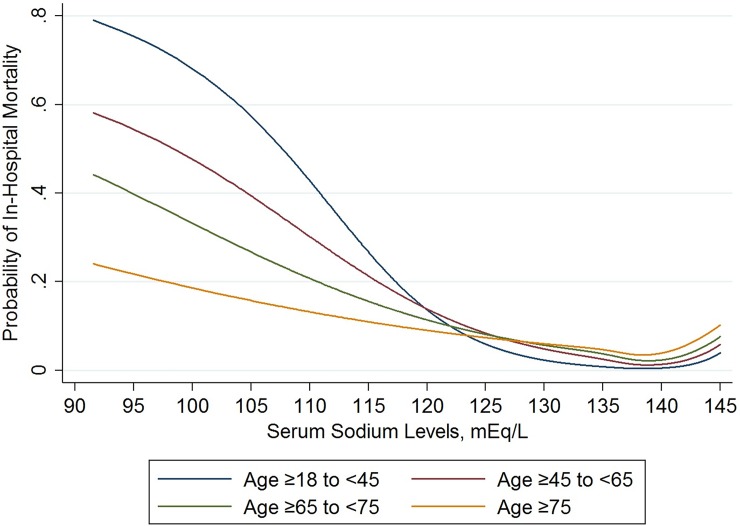
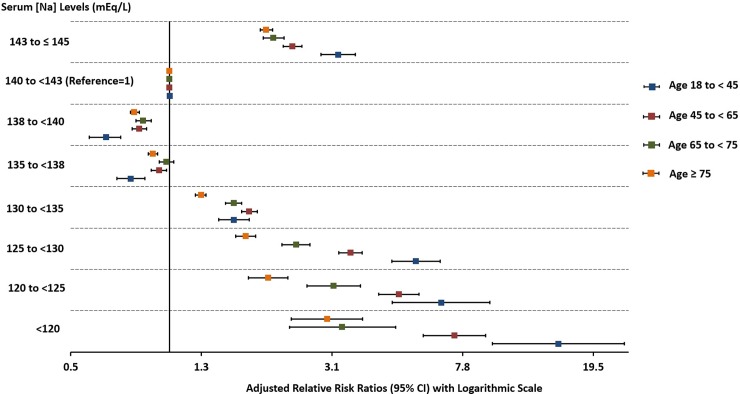
Results: At hospital admission 14.4% of hospitalized patients had serum sodium levels [Na] <135 mEq/L. In adjusted multinomial logistic regression analysis, we found that the risk of in-hospital mortality significantly increases for [Na] levels < 135 or ≥143 to ≤145 mEq/L compared to the reference interval of 140 to <143 mEq/L (p<0.001). We observed similar trends for the relationship between [Na] levels and discharge to hospice or to a nursing facility. We demonstrated that younger age groups (18 to <45, 45 to <65) had a higher risk of in-hospital mortality compared to older age groups (65 to <75, ≥75) for [Na] levels <130 mEq/L or 143 to ≤145 mEq/L (p<0.001).
Conclusions: Hyponatremia is common among hospitalized patients and is significantly associated with in-hospital mortality, discharge to hospice or to a nursing facility. The risk of death and other outcomes was more evident for [Na] <135 mEq/L. The mortality associated with low [Na] was significantly higher in younger versus older patients.
Conflict of interest statement
Figures
References
-
- Upadhyay A, Jaber BL, Madias NE. Incidence and prevalence of hyponatremia. The American journal of medicine. 2006;119(7 Suppl 1):S30–5. doi: 10.1016/j.amjmed.2006.05.005 . - DOI - PubMed
-
- Vaidya C, Ho W, Freda BJ. Management of hyponatremia: providing treatment and avoiding harm. Cleve Clin J Med. 2010;77(10):715–26. doi: 10.3949/ccjm.77a.08051 . - DOI - PubMed
-
- Hoorn EJ, Lindemans J, Zietse R. Development of severe hyponatraemia in hospitalized patients: treatment-related risk factors and inadequate management. Nephrol Dial Transplant. 2006;21(1):70–6. doi: 10.1093/ndt/gfi082 . - DOI - PubMed
-
- Gill G, Huda B, Boyd A, Skagen K, Wile D, Watson I, et al. Characteristics and mortality of severe hyponatraemia—a hospital-based study. Clin Endocrinol (Oxf). 2006;65(2):246–9. doi: 10.1111/j.1365-2265.2006.02583.x . - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
