

The role of concurrent chemotherapy for stage II nasopharyngeal carcinoma in the intensity-modulated radiotherapy era: A systematic review and meta-analysis
- PMID: 29566078
- PMCID: PMC5864049
- DOI: 10.1371/journal.pone.0194733
The role of concurrent chemotherapy for stage II nasopharyngeal carcinoma in the intensity-modulated radiotherapy era: A systematic review and meta-analysis
Abstract
Objectives: To compare clinical outcomes of concurrent chemoradiotherapy (CCRT) with those of radiotherapy alone for stage II nasopharyngeal carcinoma in the intensity-modulated radiotherapy (IMRT) era.
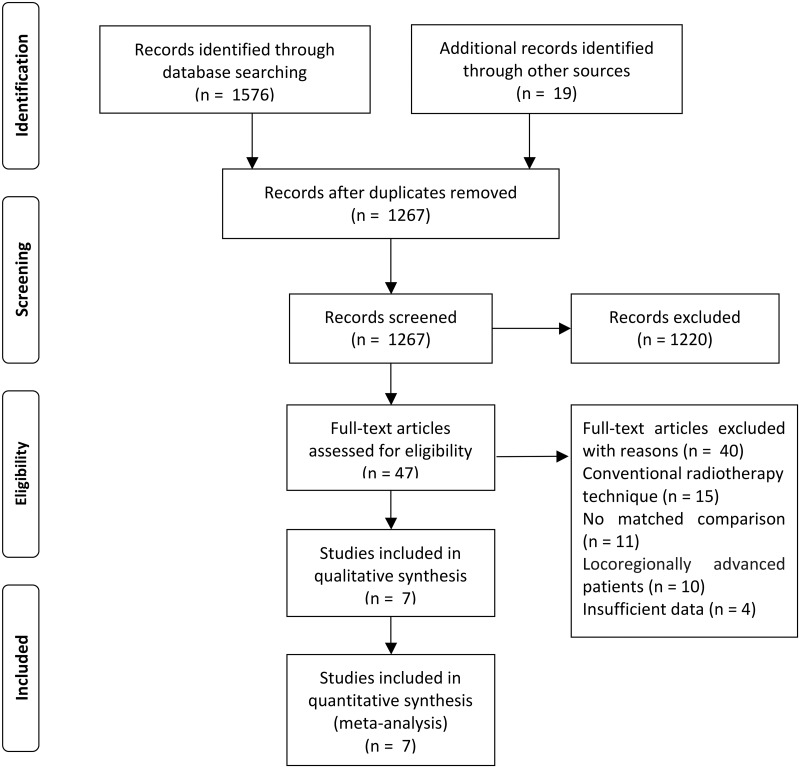
Materials and methods: We comprehensively searched PubMed, Embase, and the Cochrane Library to identify eligible studies. Overall survival (OS), progression-free survival (PFS), distant metastasis-free survival (DMFS), locoregional recurrence-free survival (LRRFS) with hazard ratios (HRs), and toxicities with odd ratios (ORs) were analyzed.
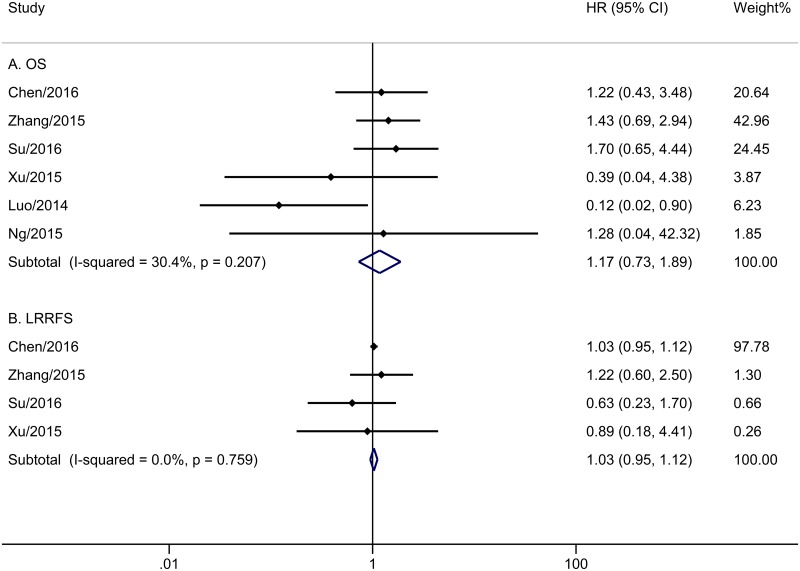
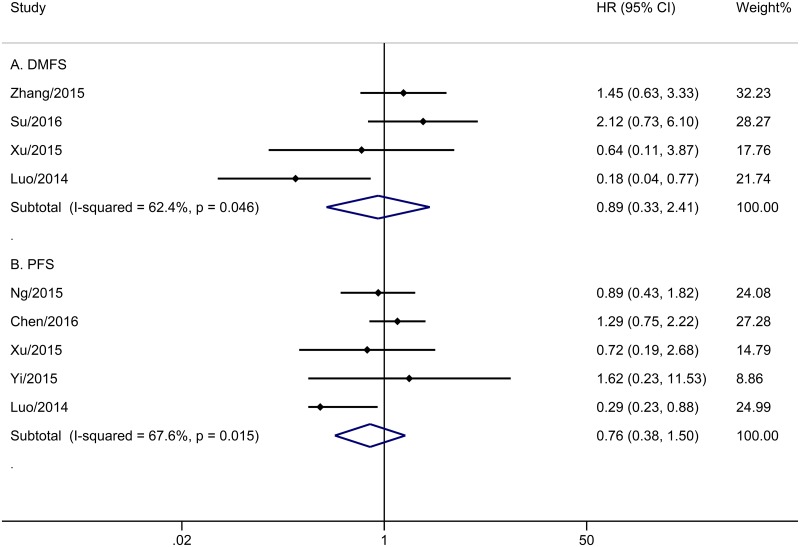
Results: A total of seven studies met the criteria, with 1302 patients who were treated with IMRT alone or IMRT plus concurrent chemotherapy. No significant survival benefit was shown by CCRT regardless of OS (HR = 1.17, 95% CI 0.73-1.89, P = 0.508), PFS (HR = 0.76, 95% CI 0.38-1.50, P = 0.430), DMFS (HR = 0.89, 95% CI 0.33-2.41, P = 0.816), or LRRFS (HR = 1.03, 95% CI 0.95-1.12, P = 0.498). Additionally, CCRT notably increased the risk of acute grade 3-4 leukopenia (OR = 4.432, 95% CI 2.195-8.952, P < 0.001), compared to IMRT alone.
Conclusion: Adding concurrent chemotherapy to IMRT led to no survival benefit and increased acute toxicity reactions for stage II nasopharyngeal carcinoma.
Conflict of interest statement
Figures
References
-
- Cao S-M, Simons MJ, Qian C-N. The prevalence and prevention of nasopharyngeal carcinoma in China. Chinese Journal of Cancer. 2011;30(2):114–9. doi: 10.5732/cjc.010.10377 - DOI - PMC - PubMed
-
- Chang ET, Adami HO. The Enigmatic Epidemiology of Nasopharyngeal Carcinoma. Cancer Epidemiology Biomarkers & Prevention. 2006;15(10):1765–77. doi: 10.1158/1055-9965.EPI-06-0353 - DOI - PubMed
-
- Chan AT, Gregoire V, Lefebvre JL, Licitra L, Hui EP, Leung SF, et al. Nasopharyngeal cancer: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2012;23 Suppl 7:vii83–5. Epub 2012/11/20. doi: 10.1093/annonc/mds266 . - DOI - PubMed
-
- NCCN Guidelines Version 2.2017 Head and Neck Cancers. https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf.
-
- Chen QY, Wen YF, Guo L, Liu H, Huang PY, Mo HY, et al. Concurrent Chemoradiotherapy vs Radiotherapy Alone in Stage II Nasopharyngeal Carcinoma: Phase III Randomized Trial. Journal of the National Cancer Institute. 2011;103(23):1761–70. doi: 10.1093/jnci/djr432 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
