

Multimodal Retinal Imaging in Incontinentia Pigmenti Including Optical Coherence Tomography Angiography: Findings From an Older Cohort With Mild Phenotype
- PMID: 29566114
- PMCID: PMC5876832
- DOI: 10.1001/jamaophthalmol.2018.0475
Multimodal Retinal Imaging in Incontinentia Pigmenti Including Optical Coherence Tomography Angiography: Findings From an Older Cohort With Mild Phenotype
Abstract
Importance: Incontinentia pigmenti (IP) is a rare, X-linked dominant disease with potentially severe ocular complications that predominantly affect the peripheral retina. However, little is known about its effects on the macula.
Objective: To describe the structural and vascular abnormalities observed in the maculas of patients with IP and to correlate these findings with peripheral pathologies.
Design, setting, and participants: Prospective, cross-sectional study at Wilmer Eye Institute, Johns Hopkins University. Five participants with a clinical diagnosis of IP were included and underwent multimodal imaging with ultra-wide-field fluorescein angiography (FA), spectral-domain optical coherence tomography (OCT), and OCT angiography.
Main outcomes and measures: The structural and vascular abnormalities observed on spectral-domain OCT and OCT angiography and their correlation with peripheral pathologies seen on ultra-wide-field FA.
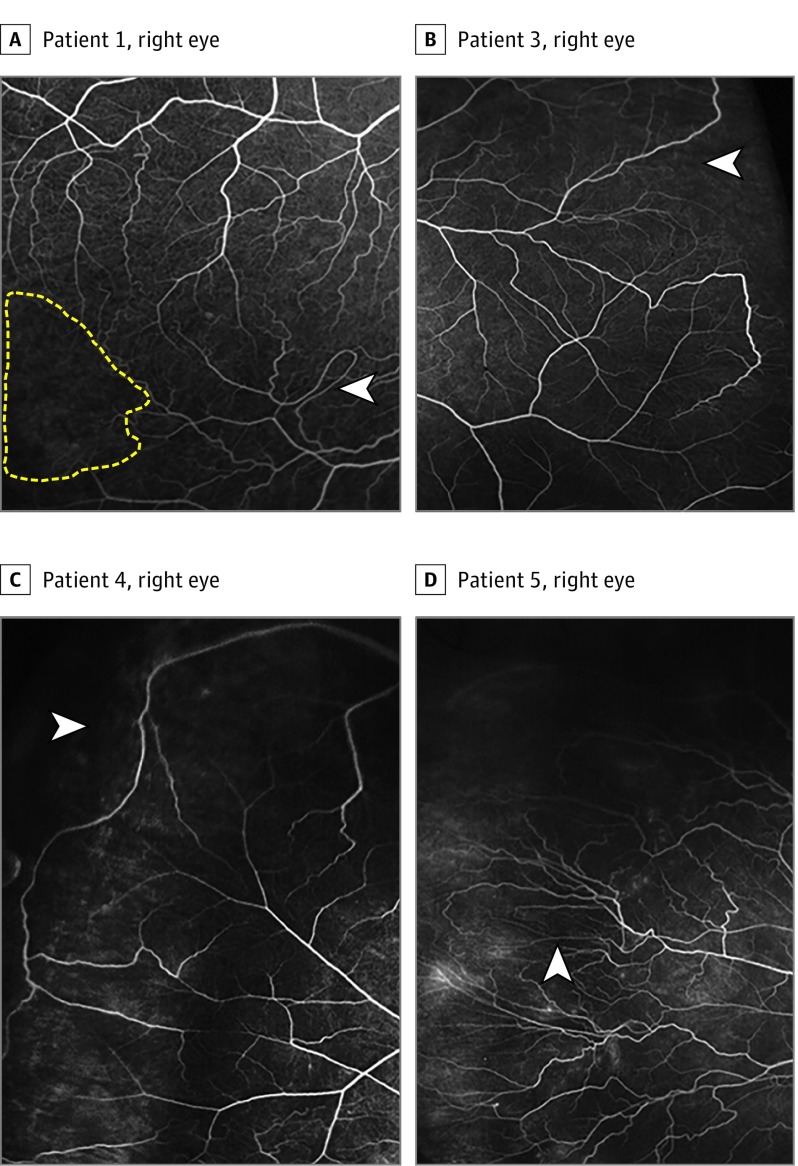
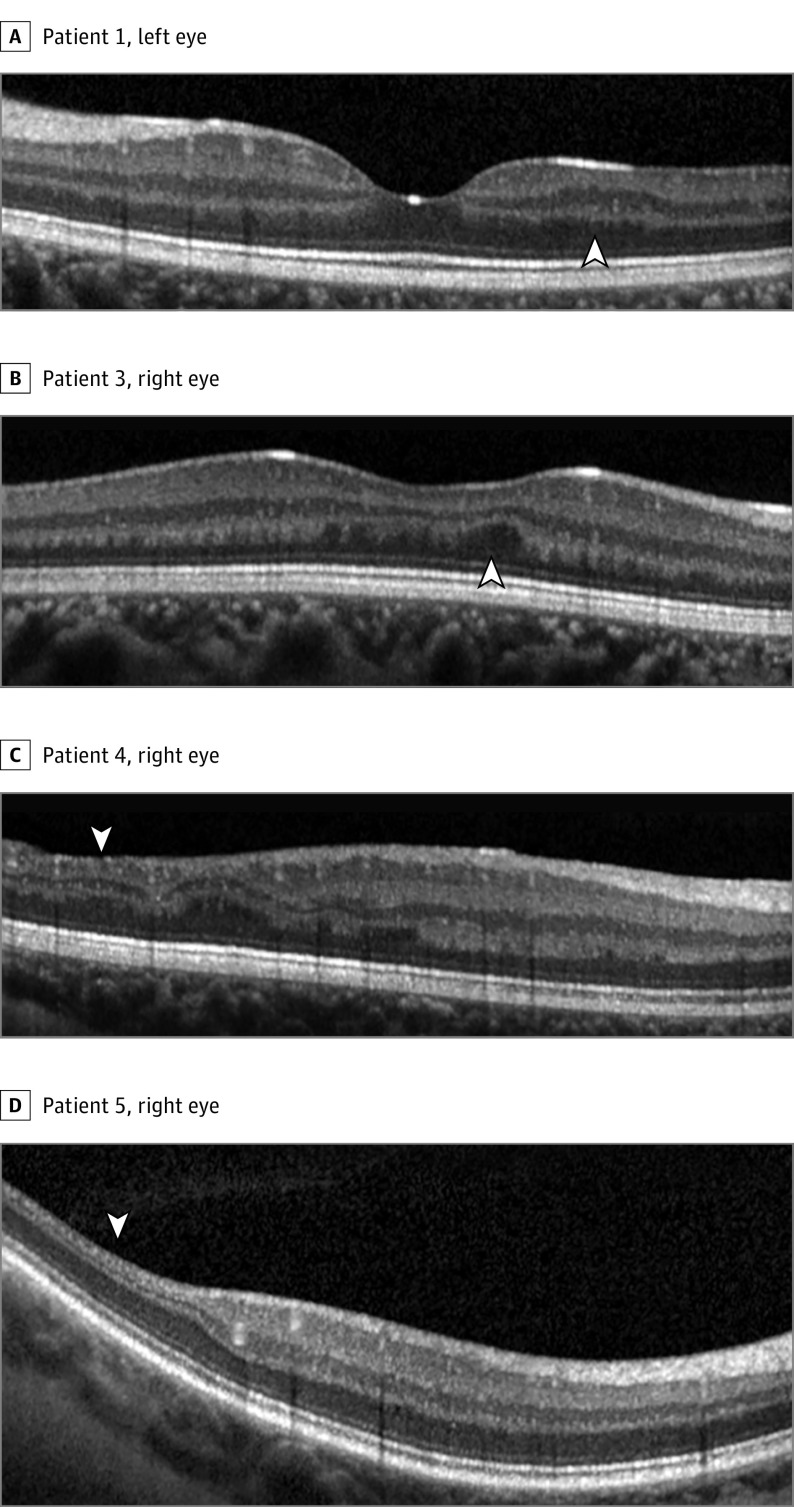
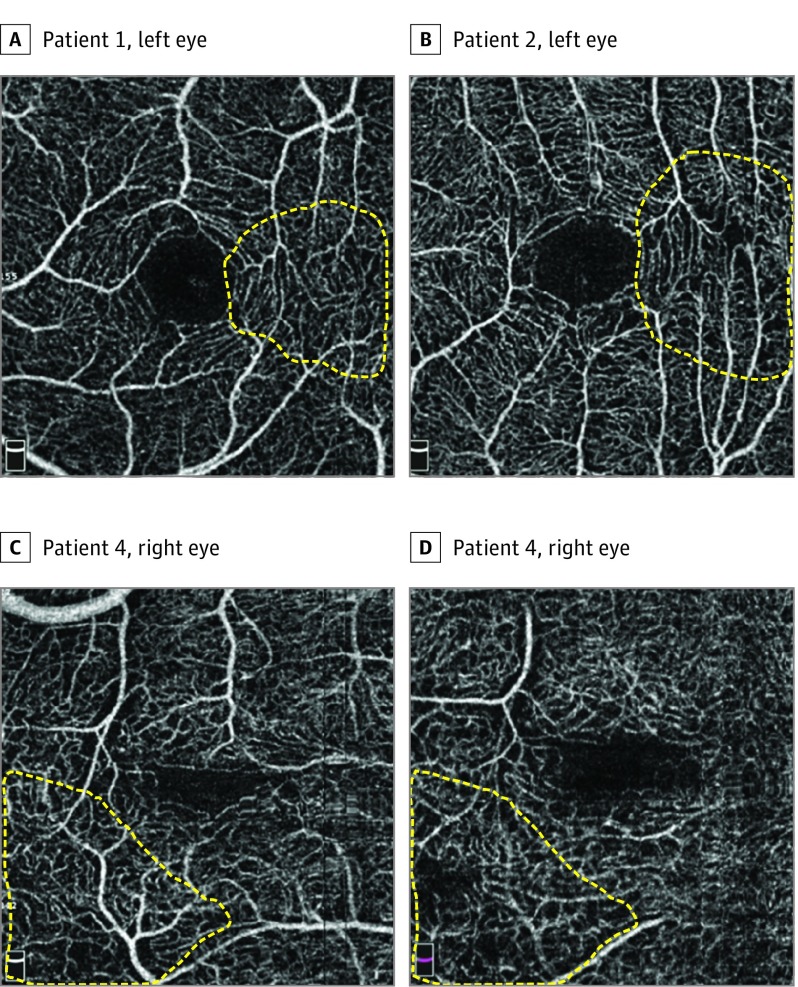
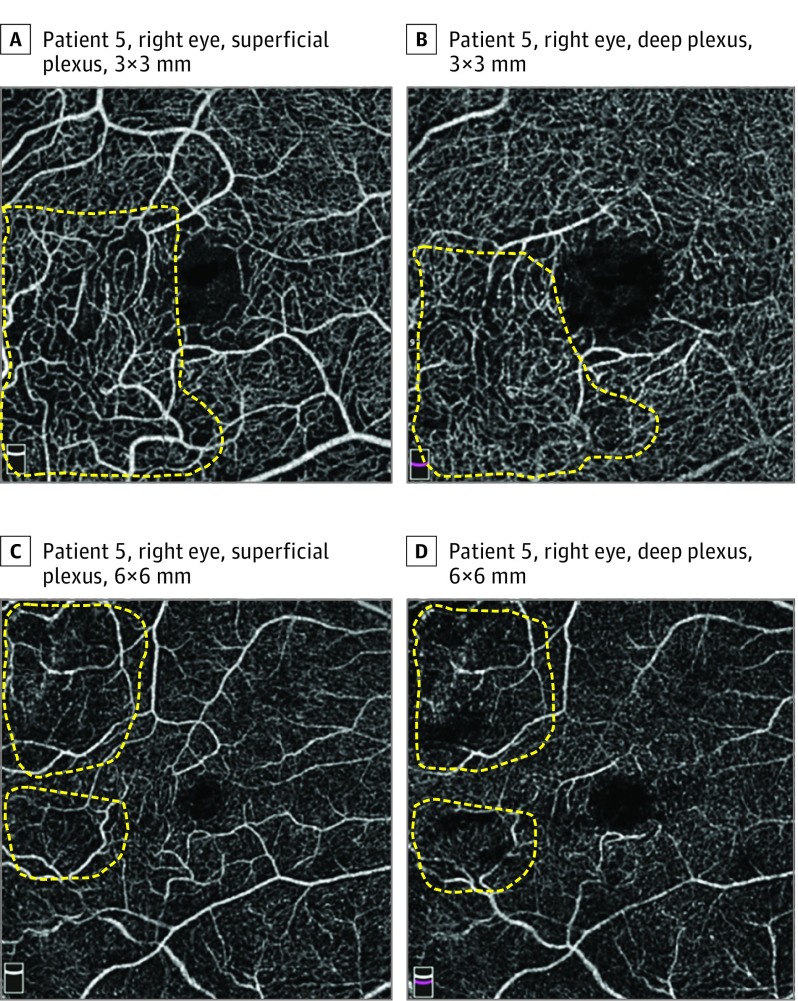
Results: A total of 9 eyes from 5 patients (median age, 20.5 years; range, 8.4-54.2 years) were included. Median Snellen visual acuity was 20/32 (range, 20/16 to 20/63). ultra-wide-field FA-identified retinal vascular abnormalities in all 7 eyes in which FA was obtained. These abnormalities included microaneurysms, areas of nonperfusion, and vascular anastomoses, most of which were peripheral to the standard view of 30° FA with peripheral sweeps. Structural abnormalities were observed in 6 eyes on spectral-domain OCT, including inner retinal thinning and irregularities in the outer plexiform layer. Optical coherence tomography angiography abnormalities were noted in all 9 eyes, including decreased vascular density, abnormal vascular loops, and flow loss in the superficial and deep plexuses, which corresponded to areas of retinal thinning on spectral-domain OCT.
Conclusions and relevance: Although our study is limited by the small sample size, the findings suggest that multimodal imaging is useful for detecting structural and vascular abnormalities that may not be apparent on ophthalmoscopy in patients with IP. Macular pathologies, especially a decrease in vascular density on OCT angiography, are common. Further studies are needed to characterize further the association between macular and peripheral abnormalities in patients with IP.
Conflict of interest statement
Figures
Similar articles
-
Child with a mild phenotype of Incontinentia Pigmenti and inner retinal dysfunction.Doc Ophthalmol. 2021 Aug;143(1):93-98. doi: 10.1007/s10633-021-09824-0. Epub 2021 Feb 13. Doc Ophthalmol. 2021. PMID: 33582953
-
Wide-Field Swept-Source OCT and Angiography in X-Linked Retinoschisis.Ophthalmol Retina. 2019 Feb;3(2):178-185. doi: 10.1016/j.oret.2018.09.006. Epub 2018 Sep 19. Ophthalmol Retina. 2019. PMID: 31014769
-
Optical Coherence Tomography Angiography and Ultra-Widefield Optical Coherence Tomography in a Child With Incontinentia Pigmenti.Ophthalmic Surg Lasers Imaging Retina. 2018 Apr 1;49(4):273-275. doi: 10.3928/23258160-20180329-11. Ophthalmic Surg Lasers Imaging Retina. 2018. PMID: 29664986 Free PMC article.
-
Incontinentia pigmenti and the eye.Curr Opin Ophthalmol. 2022 Nov 1;33(6):525-531. doi: 10.1097/ICU.0000000000000863. Epub 2022 Jul 12. Curr Opin Ophthalmol. 2022. PMID: 35819905 Review.
-
Plexus-specific retinal vascular anatomy and pathologies as seen by projection-resolved optical coherence tomographic angiography.Prog Retin Eye Res. 2021 Jan;80:100878. doi: 10.1016/j.preteyeres.2020.100878. Epub 2020 Jul 24. Prog Retin Eye Res. 2021. PMID: 32712135 Free PMC article. Review.
Cited by
-
Multimodal retinal imaging of a 6-year-old male child with incontinentia pigmenti.Indian J Ophthalmol. 2019 Jun;67(6):942-943. doi: 10.4103/ijo.IJO_192_19. Indian J Ophthalmol. 2019. PMID: 31124522 Free PMC article. No abstract available.
-
Optical Coherence Tomography Angiography in Pediatric Retinal Disorders.J Vitreoretin Dis. 2022 Jun 3;6(3):221-228. doi: 10.1177/24741264221083873. eCollection 2022 May-Jun. J Vitreoretin Dis. 2022. PMID: 37008546 Free PMC article. Review.
-
Optical Coherence Tomography and Optical Coherence Tomography Angiography in Pediatric Retinal Diseases.Diagnostics (Basel). 2023 Apr 18;13(8):1461. doi: 10.3390/diagnostics13081461. Diagnostics (Basel). 2023. PMID: 37189561 Free PMC article. Review.
-
MACULAR NEUROVASCULAR ABNORMALITIES IN A CHILD WITH INCONTINENTIA PIGMENTI ON HANDHELD OPTICAL COHERENCE TOMOGRAPHY ANGIOGRAPHY.Retin Cases Brief Rep. 2023 Sep 1;17(5):595-599. doi: 10.1097/ICB.0000000000001264. Retin Cases Brief Rep. 2023. PMID: 37643049 Free PMC article.
-
Optical coherence tomography in pediatric patients: a clinical review.Ther Adv Ophthalmol. 2020 Feb 5;12:2515841420904612. doi: 10.1177/2515841420904612. eCollection 2020 Jan-Dec. Ther Adv Ophthalmol. 2020. PMID: 32076655 Free PMC article. Review.
References
-
- Sefiani A, Abel L, Heuertz S, et al. . The gene for incontinentia pigmenti is assigned to Xq28. Genomics. 1989;4(3):427-429. - PubMed
-
- Smahi A, Courtois G, Vabres P, et al. ; The International Incontinentia Pigmenti (IP) Consortium . Genomic rearrangement in NEMO impairs NF-kappaB activation and is a cause of incontinentia pigmenti. Nature. 2000;405(6785):466-472. - PubMed
-
- Hadj-Rabia S, Froidevaux D, Bodak N, et al. . Clinical study of 40 cases of incontinentia pigmenti. Arch Dermatol. 2003;139(9):1163-1170. - PubMed
-
- Carney RG. Incontinentia pigmenti: a world statistical analysis. Arch Dermatol. 1976;112(4):535-542. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
