

Characteristics and clinical assessment of unexplained sudden cardiac arrest in the real-world setting: focus on idiopathic ventricular fibrillation
- PMID: 29566157
- PMCID: PMC5982722
- DOI: 10.1093/eurheartj/ehy098
Characteristics and clinical assessment of unexplained sudden cardiac arrest in the real-world setting: focus on idiopathic ventricular fibrillation
Abstract
Aims: Recent studies have shown that in more than half of apparently unexplained sudden cardiac arrests (SCA), a specific aetiology can be unmasked by a careful evaluation. The characteristics and the extent to which such cases undergo a systematic thorough investigation in real-life practice are unknown.
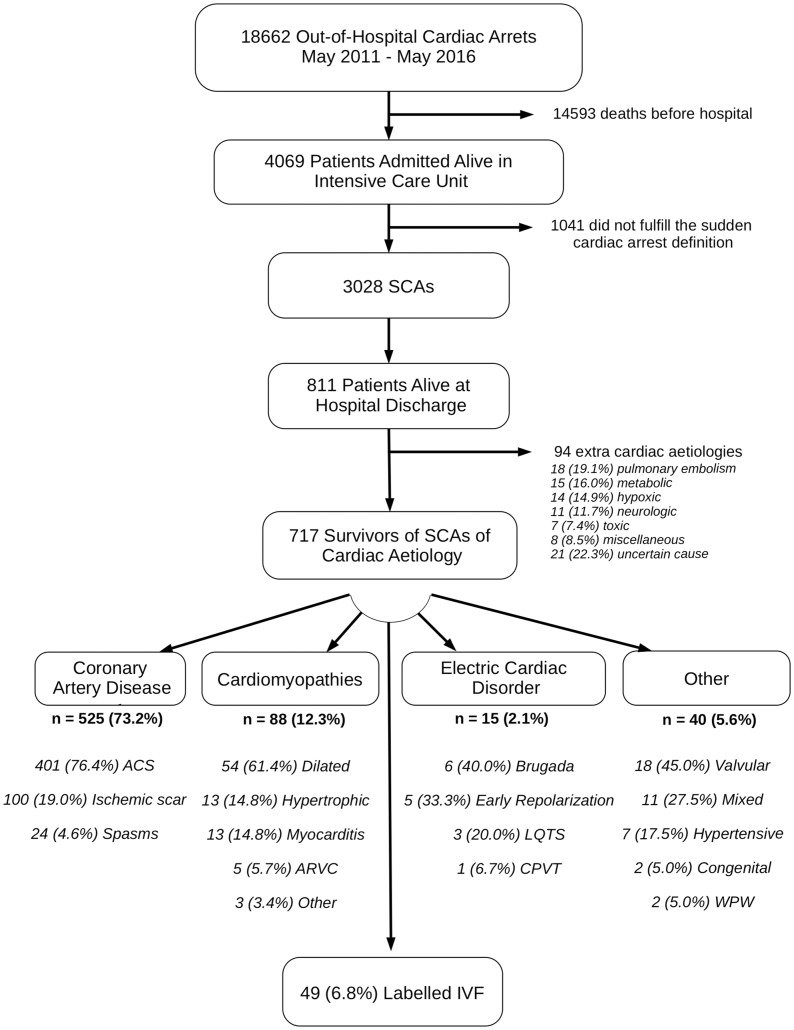
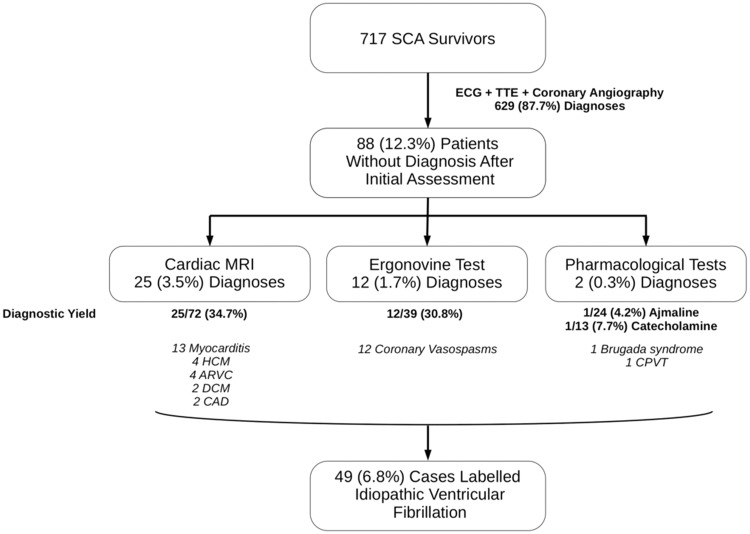
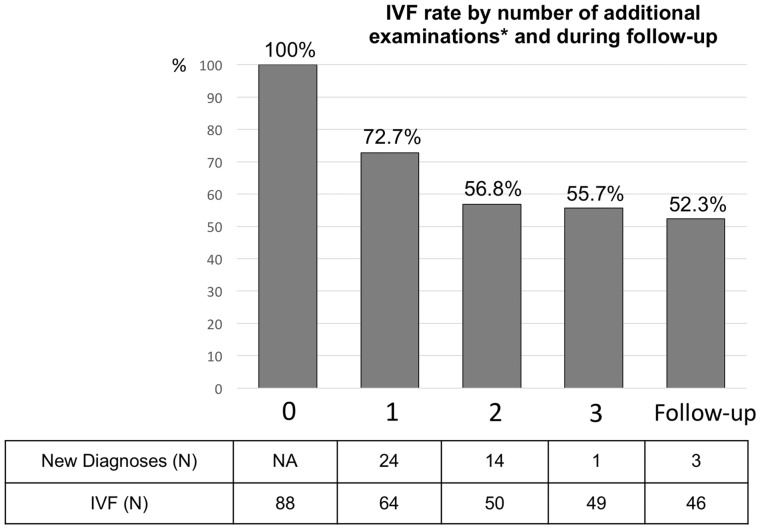
Methods and results: Data were analysed from an ongoing study, collecting all cases of out-of-hospital cardiac arrest in Paris area. Investigations performed during the index hospitalization or planned after discharge were gathered to evaluate the completeness of assessment of unexplained SCA. Between 2011 and 2016, among the 18 622 out-of-hospital cardiac arrests, 717 survivors (at hospital discharge) fulfilled the definition of cardiac SCA. Of those, 88 (12.3%) remained unexplained after electrocardiogram, echocardiography, and coronary angiography. Cardiac magnetic resonance imaging yielded the diagnosis in 25 (3.5%) cases, other investigations accounted for 14 (2.4%) additional diagnoses, and 49 (6.8%) patients were labelled as idiopathic ventricular fibrillation (IVF) (48.7 ± 15 years, 69.4% male). Among those labelled IVF, only 8 (16.3%) cases benefited from a complete workup (including pharmacological testing). Younger patients [odds ratio (OR) 6.00, 95% confidence interval (CI) 1.80-22.26] and those admitted to university centres (OR 3.60, 95% CI 1.12-12.45) were more thoroughly investigated. Genetic testing and family screening were initiated in only 9 (18.4%) and 12 (24.5%) cases, respectively.
Conclusion: Our findings suggest that complete investigations are carried out in a very low proportion of unexplained SCA. Standardized, systematic approaches need to be implemented to ensure that opportunities for specific therapies and preventive strategies (including relatives) are not missed.
Figures
Comment in
-
The importance of a comprehensive evaluation of survivors of cardiac arrest.Eur Heart J. 2018 Jun 1;39(21):1988-1991. doi: 10.1093/eurheartj/ehy160. Eur Heart J. 2018. PMID: 29584853 No abstract available.
References
-
- Fishman GI, Chugh SS, Dimarco JP, Albert CM, Anderson ME, Bonow RO, Buxton AE, Chen P-S, Estes M, Jouven X, Kwong R, Lathrop DA, Mascette AM, Nerbonne JM, O'Rourke B, Page RL, Roden DM, Rosenbaum DS, Sotoodehnia N, Trayanova NA, Zheng Z-J.. Sudden cardiac death prediction and prevention: report from a National Heart, Lung, and Blood Institute and Heart Rhythm Society Workshop. Circulation 2010;122:2335–2348. - PMC - PubMed
-
- Townsend N, Wilson L, Bhatnagar P, Wickramasinghe K, Rayner M, Nichols M.. Cardiovascular disease in Europe: epidemiological update 2016. Eur Heart J 2016;37:3232–3245. - PubMed
-
- Atlas Writing Group, Timmis A, Townsend N, Gale C, Grobbee R, Maniadakis N, Flather M, Wilkins E, Wright L, Vos R, Bax J, Blum M, Pinto F, Vardas P.. European Society of Cardiology: cardiovascular disease statistics 2017. Eur Heart J 2018;39:508–579. - PubMed
-
- Waldmann V, Bougouin W, Karam N, Albuisson J, Cariou A, Jouven X, Marijon E. Sudden cardiac death: a better understanting for a better prevention. Ann Cardiol Angeiol (Paris) 2017;66:230–238. - PubMed
-
- Behr ER, Dalageorgou C, Christiansen M, Syrris P, Hughes S, Tome Esteban MT, Rowland E, Jeffery S, McKenna WJ.. Sudden arrhythmic death syndrome: familial evaluation identifies inheritable heart disease in the majority of families. Eur Heart J 2008;29:1670–1680. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
