

Geographic assessment of access to health care in patients with cardiovascular disease in South Africa
- PMID: 29566692
- PMCID: PMC5863828
- DOI: 10.1186/s12913-018-3006-0
Geographic assessment of access to health care in patients with cardiovascular disease in South Africa
Abstract
Background: Noncommunicable diseases (NCDs) including cardiovascular diseases (CVDs), diabetes, cancer and chronic lung disease are increasingly emerging as major contributors to morbidity and mortality in developing countries. For example, in South Africa, 195 people died per day between 1997 and 2004 from CVDs related causes. Access to efficient and effective health facility and care is an important contributing factor to overall population health and addressing prognosis, care and management CVD disease burden. This study aimed to spatially evaluate geographic health care access of people diagnosed with CVD to health facilities and to evaluate the density of the existing health facility network in South Africa.
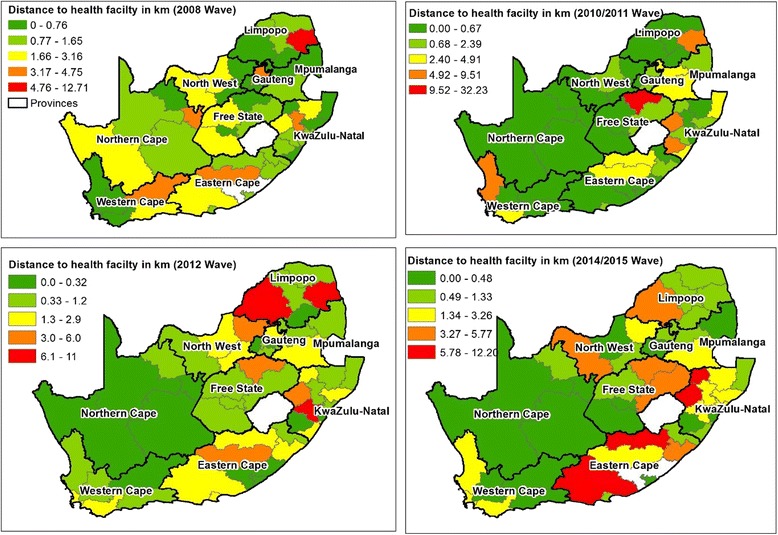
Methods: Data was obtained from the National Income Dynamics Study (NIDS) conducted in 4 waves (phases) between 2008 and 2014. The participants who responded as having heart problems that were diagnosed by a health practitioner were extracted for use in this study. Network analyst in ArcGIS ® was used to generate a least-cost path, which refers to the best path that one can travel. The residential locations of participants diagnosed with heart problems were put into the network analysis model as origins and the location of health facilities were destinations. District averages were used to protect the identity of studied participants.
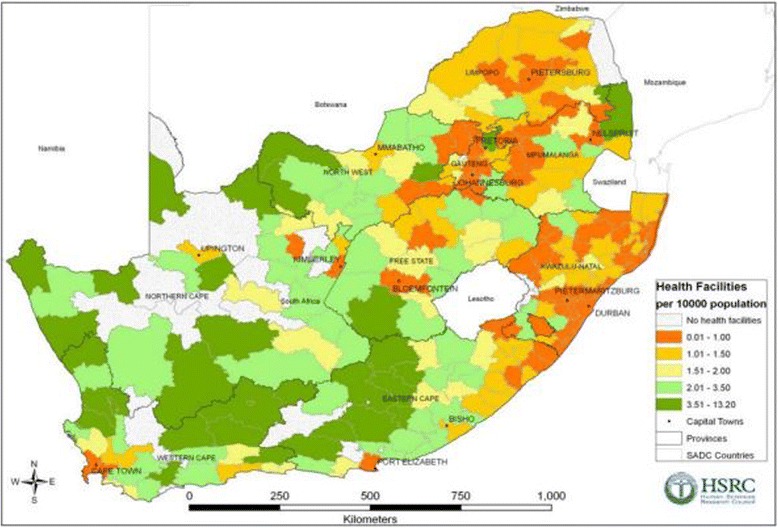
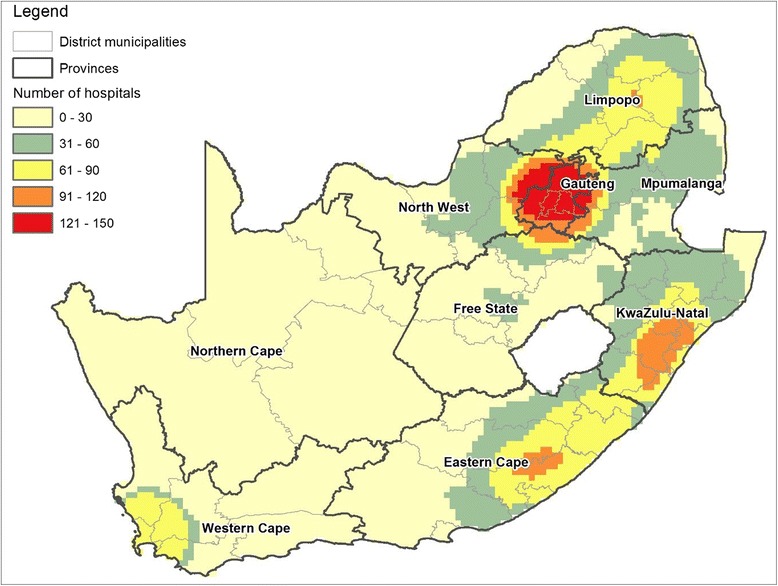
Results: There were a total of 51, 42, 43, 43 health districts out the 52 that had recorded subjects with a heart condition in the 2008, 2010-2011, 2012 and 2014-2015 waves, respectively. The mean distance from a case household to a health facility per wave was 2, 2.3, 2.1 and 2.1 km in 2008, 2010-2011 and 2014-2015 respectively. The maximum individual distances travelled per wave were 41.4 km, 40,5 km, 44,2 km and 39.6 km for the 2008, 2010-2011, 2012 and 2014-2015 waves respectively. For district level analysis, participants with CVD residing in the districts found to be among the poorest in the country travelled the longest distances. These were located in the provinces of Limpopo and KwaZulu Natal. It was also found that districts with large proportions of their population living in rural settings had among the lowest densities of health facilities. Significant percentages of study participants were exposed to numerous CVD risk factors, the commonly reported one being high blood pressure. A lack of regular exercise was also commonly reported in each of the waves.
Conclusion: A lack of accessible healthcare in already impoverished municipalities could result in an increase lack of timely diagnosis, CVD case management. This could result in increased CVD-related morbidity and mortality. GIS methods have the potential to assist national health programs to develop policies that target issues such as areas or populations being underserved by health facilities and populations that must travel long distances to receive healthcare. These policies will be key in preventing and controlling the emerging CVD burden through an accessible primary healthcare system for early detection and case management.
Keywords: Cardiovascular disease; Geographic information systems; Healthcare access.
Conflict of interest statement
Ethics approval and consent to participate
All data used in this study are secondary data from the National Income Dynamics Study (NIDS), the first national panel study in South Africa. The Southern Africa Labour and Development Research Unit (SALDRU) based in the School of Economics at the University of Cape Town was tasked with implementing this survey. The study began in 2008 and is repeated with the same household members every 2 years. Ethics for the NIDS survey was obtained from the Ethics Committee of the University of Cape Town. Adults that were willing to participate in the NIDS survey were asked to sign a consent form approved by the Ethics Committee of the University of Cape Town.
Consent for publication
Not applicable.
Competing interests
The authors declare they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- World Health Organization Cardiovascular diseases Fact Sheet Available at http://www.whoint/mediacentre/factsheets/fs317/en/. Accessed 29 Mar 2107.
-
- World Health Organization Global Health Risks Report Part 2. Available at http://www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_re.... Accessed 28 Nov 2017.
-
- Joshi R, Jan S, Wu Y, MacMahon S. Global inequalities in access to cardiovascular health care: our greatest challenge. J Am Coll Cardiol. 2008;52(23):1817–1825. - PubMed
-
- Daar AS, Singer PA, Leah Persad D, Pramming SK, Matthews DR, Beaglehole R, Bernstein A, Borysiewicz LK, Colagiuri S, Ganguly N, et al. Grand challenges in chronic non-communicable diseases. Nature. 2007;450(7169):494–496. - PubMed
-
- Mayosi BM, Flisher AJ, Lalloo UG, Sitas F, Tollman SM, Bradshaw D. The burden of non-communicable diseases in South Africa. Lancet. 374(9693):934–47. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
