

Acute exacerbation of idiopathic pulmonary fibrosis: lessons learned from acute respiratory distress syndrome?
- PMID: 29566734
- PMCID: PMC5865285
- DOI: 10.1186/s13054-018-2002-4
Acute exacerbation of idiopathic pulmonary fibrosis: lessons learned from acute respiratory distress syndrome?
Abstract
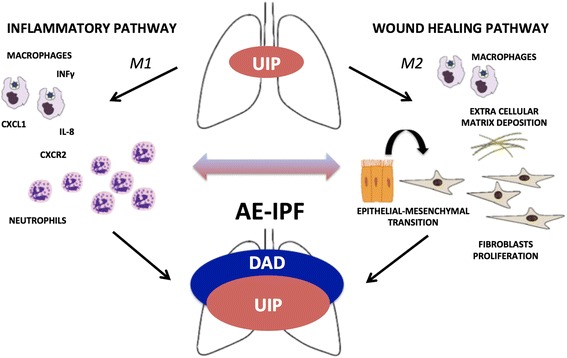
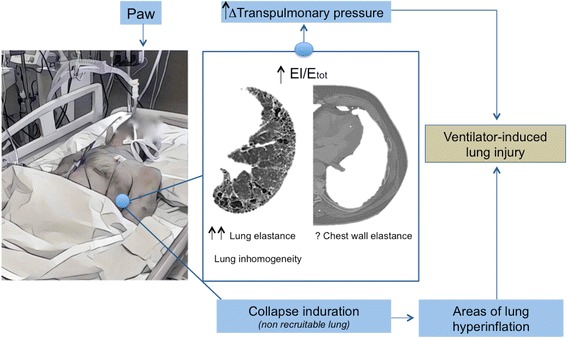
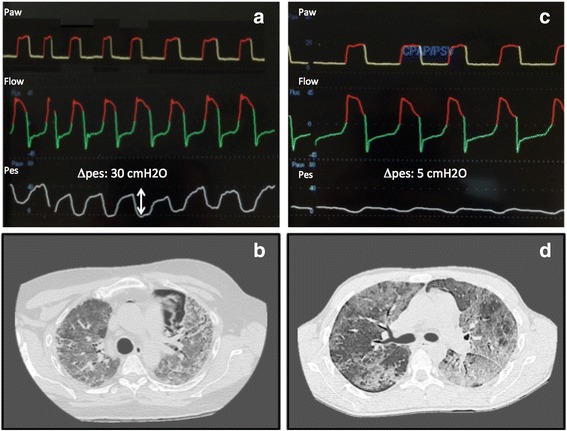
Idiopathic pulmonary fibrosis (IPF) is a fibrotic lung disease characterized by progressive loss of lung function and poor prognosis. The so-called acute exacerbation of IPF (AE-IPF) may lead to severe hypoxemia requiring mechanical ventilation in the intensive care unit (ICU). AE-IPF shares several pathophysiological features with acute respiratory distress syndrome (ARDS), a very severe condition commonly treated in this setting.A review of the literature has been conducted to underline similarities and differences in the management of patients with AE-IPF and ARDS.During AE-IPF, diffuse alveolar damage and massive loss of aeration occurs, similar to what is observed in patients with ARDS. Differently from ARDS, no studies have yet concluded on the optimal ventilatory strategy and management in AE-IPF patients admitted to the ICU. Notwithstanding, a protective ventilation strategy with low tidal volume and low driving pressure could be recommended similarly to ARDS. The beneficial effect of high levels of positive end-expiratory pressure and prone positioning has still to be elucidated in AE-IPF patients, as well as the precise role of other types of respiratory assistance (e.g., extracorporeal membrane oxygenation) or innovative therapies (e.g., polymyxin-B direct hemoperfusion). The use of systemic drugs such as steroids or immunosuppressive agents in AE-IPF is controversial and potentially associated with an increased risk of serious adverse reactions.Common pathophysiological abnormalities and similar clinical needs suggest translating to AE-IPF the lessons learned from the management of ARDS patients. Studies focused on specific therapeutic strategies during AE-IPF are warranted.
Keywords: Acute respiratory distress syndrome; Diffuse alveolar damage; Idiopathic pulmonary fibrosis; Mechanical ventilation; Respiratory failure.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors have no competing interests with any organization or entity with a financial interest in competition with the subject, matter, or materials discussed in the manuscript.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Prognostic evaluation by oxygenation with positive end-expiratory pressure in acute exacerbation of idiopathic pulmonary fibrosis: A retrospective cohort study.Clin Respir J. 2018 Mar;12(3):895-903. doi: 10.1111/crj.12602. Epub 2017 Jan 12. Clin Respir J. 2018. PMID: 28026113
-
Inspiratory Effort and Respiratory Mechanics in Patients with Acute Exacerbation of Idiopathic Pulmonary fibrosis: A Preliminary Matched Control Study.Pulmonology. 2023 Nov-Dec;29(6):469-477. doi: 10.1016/j.pulmoe.2022.08.004. Epub 2022 Sep 28. Pulmonology. 2023. PMID: 36180352
-
Noninvasive ventilation in acute exacerbation of idiopathic pulmonary fibrosis.Intern Med. 2010;49(15):1509-14. doi: 10.2169/internalmedicine.49.3222. Epub 2010 Aug 2. Intern Med. 2010. PMID: 20686281
-
Acute Respiratory Distress Syndrome: Advances in Diagnosis and Treatment.JAMA. 2018 Feb 20;319(7):698-710. doi: 10.1001/jama.2017.21907. JAMA. 2018. PMID: 29466596 Review.
-
Mechanical ventilation in the management of acute respiratory distress syndrome.Semin Dial. 2006 Nov-Dec;19(6):517-24. doi: 10.1111/j.1525-139X.2006.00215.x. Semin Dial. 2006. PMID: 17150053 Review.
Cited by
-
Quantitative CT-analysis of over aerated lung tissue and correlation with fibrosis extent in patients with idiopathic pulmonary fibrosis.Respir Res. 2024 Oct 5;25(1):359. doi: 10.1186/s12931-024-02970-4. Respir Res. 2024. PMID: 39369240 Free PMC article.
-
The Impact of Chronic Comorbidities on Outcomes in Acute Exacerbations of Idiopathic Pulmonary Fibrosis.Life (Basel). 2024 Jan 21;14(1):156. doi: 10.3390/life14010156. Life (Basel). 2024. PMID: 38276285 Free PMC article.
-
Acute exacerbation of idiopathic pulmonary fibrosis a narrative review primary focus on treatments.J Thorac Dis. 2024 Jul 30;16(7):4727-4741. doi: 10.21037/jtd-23-1565. Epub 2024 Jul 11. J Thorac Dis. 2024. PMID: 39144320 Free PMC article. Review.
-
Elevated Expression of Growth Differentiation Factor-15 Is Associated With Acute Exacerbation of Idiopathic Pulmonary Fibrosis.Front Immunol. 2022 Jun 15;13:891448. doi: 10.3389/fimmu.2022.891448. eCollection 2022. Front Immunol. 2022. PMID: 35784345 Free PMC article.
-
Differences between Acute Exacerbations of Idiopathic Pulmonary Fibrosis and Other Interstitial Lung Diseases.Diagnostics (Basel). 2021 Sep 6;11(9):1623. doi: 10.3390/diagnostics11091623. Diagnostics (Basel). 2021. PMID: 34573965 Free PMC article.
References
-
- Raghu G, Collard HR, Egan JJ, Martinez FJ, Behr J, Brown KK, Colby TV, Cordier JF, Flaherty KR, Lasky JA, Lynch DA, Ryu JH, Swigris JJ, Wells AU, Ancochea J, Bouros D, Carvalho C, Costabel U, Ebina M, Hansell DM, Johkoh T, Kim DS, King TE, Jr, Kondoh Y, Myers J, Müller NL, Nicholson AG, Richeldi L, Selman M, Dudden RF, Griss BS, Protzko SL, Schünemann HJ, ATS/ERS/JRS/ALAT Committee on Idiopathic Pulmonary Fibrosis An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med. 2011;183(6):788–824. doi: 10.1164/rccm.2009-040GL. - DOI - PMC - PubMed
-
- Collard HR, Moore BB, Flaherty KR, Brown KK, Kaner RJ, King TE, Jr, Lasky JA, Loyd JE, Noth I, Olman MA, Raghu G, Roman J, Ryu JH, Zisman DA, Hunninghake GW, Colby TV, Egan JJ, Hansell DM, Johkoh T, Kaminski N, Kim DS, Kondoh Y, Lynch DA, Müller-Quernheim J, Myers JL, Nicholson AG, Selman M, Toews GB, Wells AU, Martinez FJ. Idiopathic Pulmonary Fibrosis Clinical Research Network Investigators. Acute exacerbations of idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2007;176(7):636–643. doi: 10.1164/rccm.200703-463PP. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
