

Variations in Practice Patterns and Consistency With Published Guidelines for Balloon Aortic and Pulmonary Valvuloplasty: An Analysis of Data From the IMPACT Registry
- PMID: 29566797
- PMCID: PMC6156789
- DOI: 10.1016/j.jcin.2018.01.253
Variations in Practice Patterns and Consistency With Published Guidelines for Balloon Aortic and Pulmonary Valvuloplasty: An Analysis of Data From the IMPACT Registry
Abstract
Objectives: The authors sought to study variation in the practice of balloon aortic (BAV) and pulmonary valvuloplasty (BPV).
Background: The IMPACT (IMProving Adult and Congenital Treatment) registry provides an opportunity to study practice variation in transcatheter interventions for congenital heart disease.
Methods: The authors studied BAV and BPV in the IMPACT registry from January 1, 2011, to September 30, 2015, using hierarchical multivariable models to measure hospital-level variation in: 1) the distribution of indications for intervention; and 2) in cases with "high resting gradient" as the indication, consistency with published guidelines.
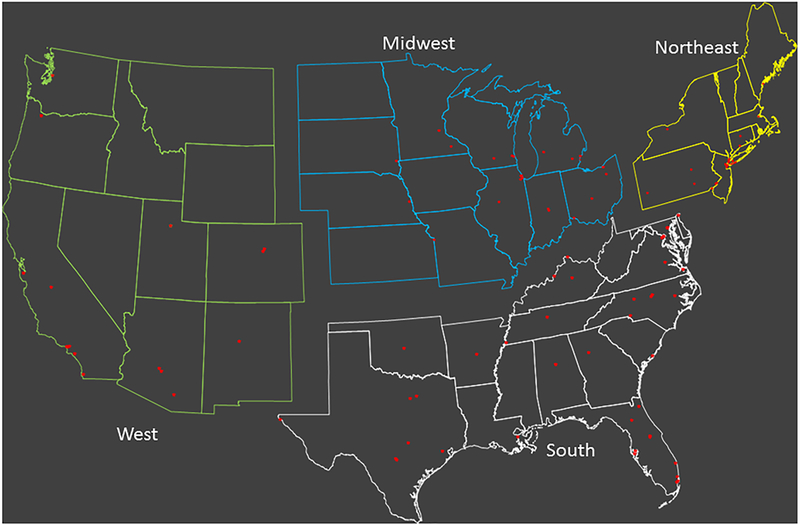
Results: A total of 1,071 BAV cases at 60 hospitals and 2,207 BPV cases at 75 hospitals were included. The indication for BAV was high resting gradient in 82%, abnormal stress test or electrocardiogram (2%), left ventricular dysfunction (11%), and symptoms (5%). Indications for BPV were high resting gradient in 82%, right-left shunt (6%), right ventricular dysfunction (7%), and symptoms (5%). No association between hospital characteristics and distribution of indications was demonstrated. Among interventions performed for "high resting gradient," there was significant adjusted hospital-level variation in the rates of cases performed consistently with guidelines. For BAV, significant differences were seen across census regions, with hospitals in the East and South more likely to practice consistently than those in the Midwest and West (p = 0.005). For BPV, no association was found between hospital factors and rates of consistent practice, but there was significant interhospital variation (median rate ratio: 1.4; 95% confidence interval: 1.2 to 1.6; p < 0.001).
Conclusions: There is measurable hospital-level variation in the practice of BAV and BPV. Further research is necessary to determine whether this affects outcomes or resource use.
Keywords: cardiac catheterization; congenital heart disease; health services research; outcomes research.
Copyright © 2018 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures


Comment in
-
What Is the IMPACT of Practice Variation in Congenital Interventional Cardiology?JACC Cardiovasc Interv. 2018 Mar 26;11(6):539-540. doi: 10.1016/j.jcin.2018.02.010. JACC Cardiovasc Interv. 2018. PMID: 29566798 No abstract available.
Similar articles
-
Acute Success of Balloon Aortic Valvuloplasty in the Current Era: A National Cardiovascular Data Registry Study.JACC Cardiovasc Interv. 2017 Sep 11;10(17):1717-1726. doi: 10.1016/j.jcin.2017.08.001. JACC Cardiovasc Interv. 2017. PMID: 28882282
-
Diminished left ventricular function is associated with poor mid-term outcomes in neonates after balloon aortic valvuloplasty.Catheter Cardiovasc Interv. 2012 Dec 1;80(7):1190-9. doi: 10.1002/ccd.23500. Epub 2012 Apr 17. Catheter Cardiovasc Interv. 2012. PMID: 22511546
-
Outcomes for balloon pulmonary valvuloplasty in adults: comparison with a concurrent pediatric cohort.Catheter Cardiovasc Interv. 2013 Nov 1;82(5):811-5. doi: 10.1002/ccd.24973. Epub 2013 Jul 11. Catheter Cardiovasc Interv. 2013. PMID: 23613310
-
The effect of multiple-inflation balloon aortic valvuloplasty.Heart Vessels. 2020 Nov;35(11):1557-1562. doi: 10.1007/s00380-020-01626-9. Epub 2020 May 30. Heart Vessels. 2020. PMID: 32474647
-
Evolution of percutaneous balloon aortic valvuloplasty in the treatment of patients with aortic stenosis.Minerva Med. 2012 Dec;103(6):415-29. Minerva Med. 2012. PMID: 23229364 Review.
Cited by
-
Failure to Rescue as an Outcome Metric for Pediatric and Congenital Cardiac Catheterization Laboratory Programs: Analysis of Data From the IMPACT Registry.J Am Heart Assoc. 2019 Nov 5;8(21):e013151. doi: 10.1161/JAHA.119.013151. Epub 2019 Oct 17. J Am Heart Assoc. 2019. PMID: 31619106 Free PMC article.
-
Resource Utilization in the First 2 Years Following Operative Correction for Tetralogy of Fallot: Study Using Data From the Optum's De-Identified Clinformatics Data Mart Insurance Claims Database.J Am Heart Assoc. 2020 Aug 4;9(15):e016581. doi: 10.1161/JAHA.120.016581. Epub 2020 Jul 21. J Am Heart Assoc. 2020. PMID: 32691679 Free PMC article.
-
Interhospital Variation in the Costs of Pediatric/Congenital Cardiac Catheterization Laboratory Procedures: Analysis of Data From the Pediatric Health Information Systems Database.J Am Heart Assoc. 2019 May 7;8(9):e011543. doi: 10.1161/JAHA.118.011543. J Am Heart Assoc. 2019. PMID: 31023121 Free PMC article.
-
Adherence with lipid screening guidelines in standard- and high-risk children and adolescents.Am Heart J. 2021 Feb;232:39-46. doi: 10.1016/j.ahj.2020.10.058. Epub 2020 Oct 24. Am Heart J. 2021. PMID: 33229294 Free PMC article.
-
Trends in transcatheter and operative closure of patent ductus arteriosus in neonatal intensive care units: Analysis of data from the Pediatric Health Information Systems Database.Am Heart J. 2019 Nov;217:121-130. doi: 10.1016/j.ahj.2019.08.009. Epub 2019 Aug 17. Am Heart J. 2019. PMID: 31654942 Free PMC article.
References
-
- Fonarow GC, Yancy CW, Heywood JT, ADHERE Scientific Advisory Committee, Study Group, and Investigators. Adherence to heart failure quality-of-care indicators in US hospitals: analysis of the ADHERE Registry. Arch. Intern. Med 2005;165:1469–1477. - PubMed
-
- Hira RS, Kennedy K, Jneid H, et al. Frequency and practice-level variation in inappropriate and nonrecommended prasugrel prescribing: insights from the NCDR PINNACLE registry. J Am Coll Cardiol 2014;63:2876–2877. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
