

Effect of diabetes duration and glycaemic control on 14-year cause-specific mortality in Mexican adults: a blood-based prospective cohort study
- PMID: 29567074
- PMCID: PMC5966587
- DOI: 10.1016/S2213-8587(18)30050-0
Effect of diabetes duration and glycaemic control on 14-year cause-specific mortality in Mexican adults: a blood-based prospective cohort study
Abstract
Background: Diabetes is a cause of at least a third of all deaths in Mexican adults aged 35-74 years, with the excess mortality due mainly to vascular disease, renal disease, infection, and acute diabetic crises. We aimed to analyse the effect of diabetes duration and glycaemic control on death rate ratios (RRs) for these causes and to assess the relevance to cause-specific mortality of undiagnosed diabetes.
Methods: About 100 000 women and 50 000 men aged 35 years or older from Mexico City were recruited into a blood-based prospective study between April 14, 1998, and Sept 28, 2004, and followed up until Jan 1, 2016, for cause-specific mortality. Participants who, at recruitment, reported any chronic disease other than diabetes and those who had missing data for HbA1c or diabetes duration were excluded. We used Cox models to estimate the associations of undiagnosed or previously diagnosed diabetes (almost all type 2) with risk of mortality from vascular disease, renal disease, and infection, exploring among those with previously diagnosed diabetes the independent relevance of diabetes duration (<5 years, ≥5 to <10 years, or ≥10 years) and HbA1c (<9%, ≥9% to <11%, or ≥11%). We also estimated the association of HbA1c with mortality in participants without diabetes at recruitment.
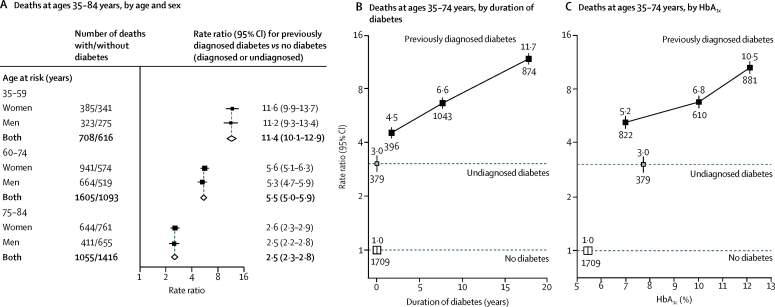
Findings: 133 662 participants were aged 35-74 years and had complete data and no other chronic disease. 16 940 (13%) had previously diagnosed diabetes, 6541 (5%) had undiagnosed diabetes, and 110 181 (82%) had no diabetes. Among participants with previously diagnosed diabetes, glycaemic control was poor (median HbA1c 8·9% [IQR 7·0-10·9]), and was worse in those with longer duration of disease at recruitment. Compared with participants without diabetes, the death RRs at ages 35-74 years for the combination of vascular, renal, or infectious causes were 3·0 (95% CI 2·7-3·4) in those with undiagnosed diabetes, 4·5 (4·0-5·0) for the 5042 participants with a diabetes duration of less than 5 years, 6·6 (6·1-7·1) for the 7713 participants with a duration of 5 years to less than 10 years, and 11·7 (10·7-12·7) for the 4185 participants with a duration of at least 10 years. Similarly, the death RRs were 5·2 (4·8-5·7) for those with HbA1c less than 9%, 6·8 (6·2-7·4) for those with HbA1c of 9% to less than 11%, and 10·5 (9·7-11·5) for those with HbA1c of at least 11%. Diabetes was not strongly associated with the combination of deaths from other causes apart from acute glycaemic crises. Among participants without diabetes, higher HbA1c was not positively related to mortality.
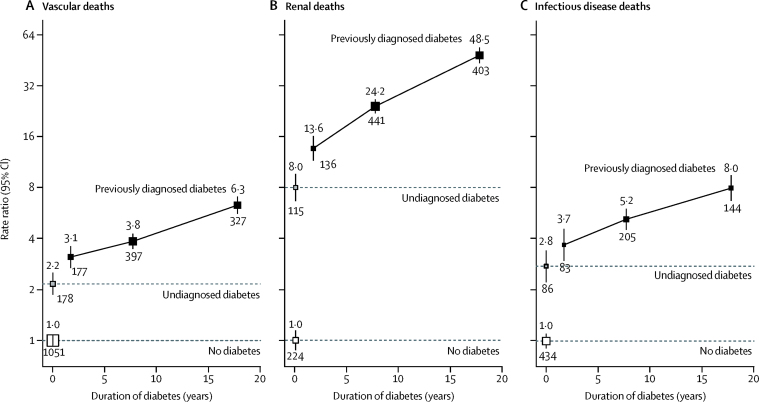
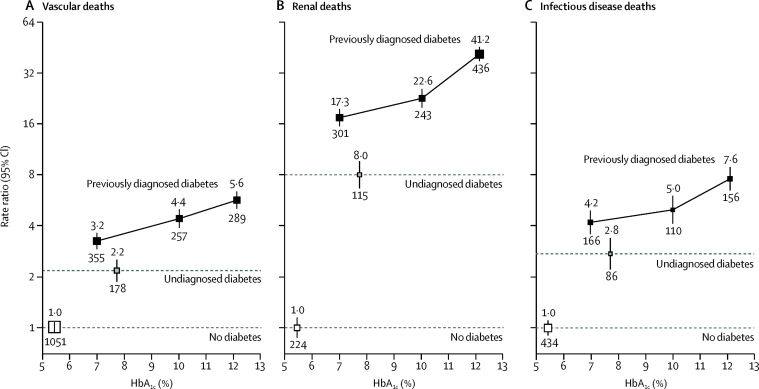
Interpretation: In Mexico, the rates of death from causes strongly associated with diabetes increased steeply with duration of diabetes and were higher still among people with poor glycaemic control. Delaying the onset of type 2 diabetes, as well as improving its treatment, is essential to reduce premature adult mortality in Mexico.
Funding: Wellcome Trust, the Mexican Health Ministry, the Mexican National Council of Science and Technology, Cancer Research UK, British Heart Foundation, and the UK Medical Research Council Population Health Research Unit.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Diabetes duration, HbA1c, and cause-specific mortality in Mexico.Lancet Diabetes Endocrinol. 2018 Jun;6(6):429-431. doi: 10.1016/S2213-8587(18)30098-6. Epub 2018 Mar 19. Lancet Diabetes Endocrinol. 2018. PMID: 29567073 No abstract available.
Similar articles
-
Prediabetes as a risk factor for all-cause and cause-specific mortality: a prospective analysis of 115,919 adults without diabetes in Mexico City.medRxiv [Preprint]. 2024 Apr 16:2024.04.15.24305840. doi: 10.1101/2024.04.15.24305840. medRxiv. 2024. PMID: 38699295 Free PMC article. Preprint.
-
Educational and social inequalities and cause-specific mortality in Mexico City: a prospective study.Lancet Public Health. 2023 Sep;8(9):e670-e679. doi: 10.1016/S2468-2667(23)00153-6. Lancet Public Health. 2023. PMID: 37633676 Free PMC article.
-
Diabetes and Cause-Specific Mortality in Mexico City.N Engl J Med. 2016 Nov 17;375(20):1961-1971. doi: 10.1056/NEJMoa1605368. N Engl J Med. 2016. PMID: 27959614 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Repaglinide : a pharmacoeconomic review of its use in type 2 diabetes mellitus.Pharmacoeconomics. 2004;22(6):389-411. doi: 10.2165/00019053-200422060-00005. Pharmacoeconomics. 2004. PMID: 15099124 Review.
Cited by
-
Cost-effectiveness of the use of the continuous subcutaneous insulin infusion pump versus daily multiple injections in type 1 diabetes adult patients at the Mexican Institute of Social Security.Cost Eff Resour Alloc. 2019 Sep 3;17:19. doi: 10.1186/s12962-019-0187-2. eCollection 2019. Cost Eff Resour Alloc. 2019. PMID: 31507338 Free PMC article.
-
The mortality in infectious inpatients with type 2 diabetes compared with non-diabetic population: Infection in type 2 diabetes.Medicine (Baltimore). 2019 Jun;98(24):e16025. doi: 10.1097/MD.0000000000016025. Medicine (Baltimore). 2019. PMID: 31192954 Free PMC article.
-
Factors associated with glycemic control among South African adult residents of Mkhondo municipality living with diabetes mellitus.Medicine (Baltimore). 2020 Nov 25;99(48):e23467. doi: 10.1097/MD.0000000000023467. Medicine (Baltimore). 2020. PMID: 33235135 Free PMC article.
-
Clinical factors influencing knowledge and self-care practice among adults with type 2 diabetes mellitus.Nurs Open. 2023 Apr;10(4):2492-2500. doi: 10.1002/nop2.1506. Epub 2022 Dec 4. Nurs Open. 2023. PMID: 36464636 Free PMC article.
-
Association of Kidney Function With NMR-Quantified Lipids, Lipoproteins, and Metabolic Measures in Mexican Adults.J Clin Endocrinol Metab. 2021 Sep 27;106(10):2828-2839. doi: 10.1210/clinem/dgab497. J Clin Endocrinol Metab. 2021. PMID: 34216216 Free PMC article.
References
-
- International Diabetes Federation . 8th edn. International Diabetes Federation; Brussels: 2017. IDF Diabetes Atlas.http://www.diabetesatlas.org/resources/2017-atlas.html (accessed Dec 29, 2017).
-
- Zoungas S, Woodward M, Li Q. Impact of age, age at diagnosis and duration of diabetes on the risk of macrovascular and microvascular complications and death in type 2 diabetes. Diabetologia. 2014;57:2465–2474. - PubMed
-
- Wannamethee SG, Shaper AG, Whincup PH, Lennon L, Sattar N. Impact of diabetes on cardiovascular disease risk and all-cause mortality in older men: influence of age at onset, diabetes duration, and established and novel risk factors. Arch Intern Med. 2011;171:404–410. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
