

Transforaminal Lumbar Puncture: An Alternative Technique in Patients with Challenging Access
- PMID: 29567652
- PMCID: PMC7410647
- DOI: 10.3174/ajnr.A5596
Transforaminal Lumbar Puncture: An Alternative Technique in Patients with Challenging Access
Abstract
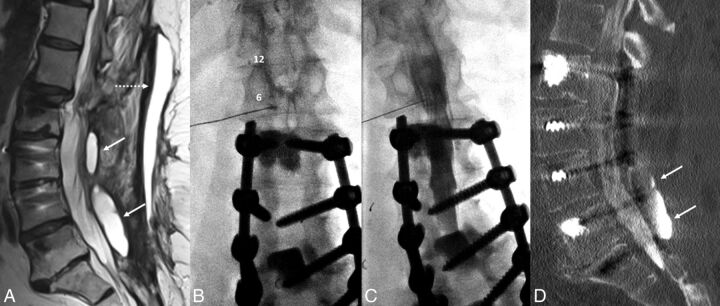
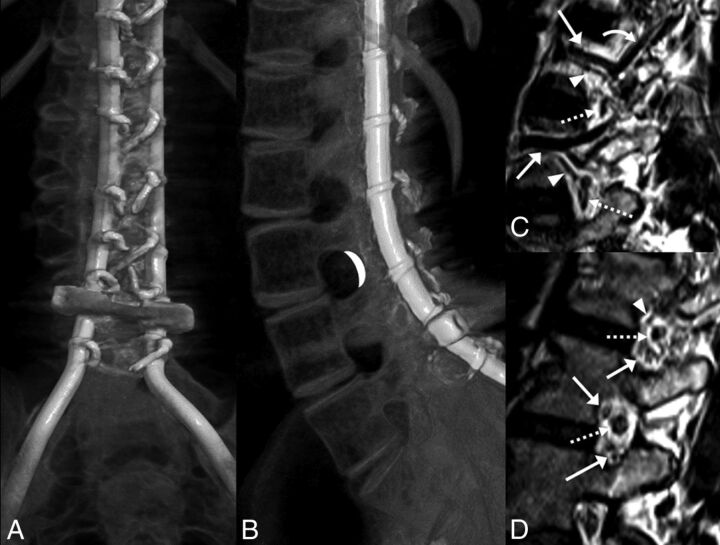
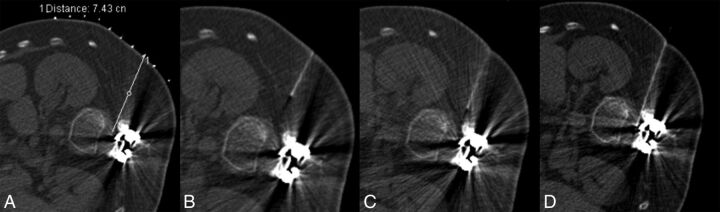
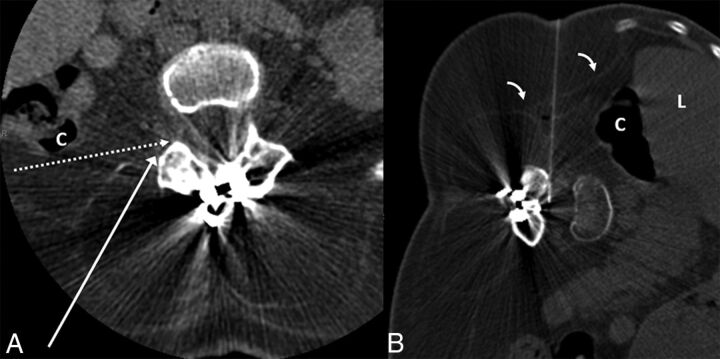
Interlaminar lumbar puncture and cervical puncture may not be ideal in all circumstances. Recently, we have used a transforaminal approach in selected situations. Between May 2016 and December 2017, twenty-six transforaminal lumbar punctures were performed in 9 patients (25 CT-guided, 1 fluoroscopy-guided). Seven had spinal muscular atrophy and were referred for intrathecal nusinersen administration. In 2, CT myelography was performed via transforaminal lumbar puncture. The lumbar posterior elements were completely fused in 8, and there was an overlying abscess in 1. The L1-2 level was used in 2; the L2-3 level, in 10; the L3-4 level, in 12; and the L4-5 level, in 2 procedures. Post-lumbar puncture headache was observed on 4 occasions, which resolved without blood patching. One patient felt heat and pain at the injection site that resolved spontaneously within hours. One patient had radicular pain that resolved with conservative treatment. Transforaminal lumbar puncture may become an effective alternative to classic interlaminar lumbar puncture or cervical puncture.
© 2018 by American Journal of Neuroradiology.
Figures
References
-
- Gibbs WN, Skalski MR, Kim PE, et al. . C1–2 puncture: a safe, efficacious, and potentially underused technique. Neurographics 2017;7:1–8 10.3174/ng.1170183 - DOI
-
- Pomerantz SR, Buchbinder B, Hirsch JA. Suboccipital puncture of the cisterna magna under CT-guidance with intravenous enhancement in order to circumvent anomalous course of posterior inferior cerebellar artery (PICA). In: Proceedings of the American Society of Spine Radiology Annual Symposium, San Juan, Puerto Rico February 24–27, 2005
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources