

Moderate-to-Vigorous Physical Activity and All-Cause Mortality: Do Bouts Matter?
- PMID: 29567764
- PMCID: PMC5907548
- DOI: 10.1161/JAHA.117.007678
Moderate-to-Vigorous Physical Activity and All-Cause Mortality: Do Bouts Matter?
Erratum in
-
Moderate-to-Vigorous Physical Activity and All-Cause Mortality: Do Bouts Matter?J Am Heart Assoc. 2018 Dec 4;7(23):e03713. doi: 10.1161/JAHA.118.002247. J Am Heart Assoc. 2018. PMID: 30511899 Free PMC article. No abstract available.
Abstract
Background: The 2008 Physical Activity Guidelines for Americans recommends that adults accumulate moderate-to-vigorous physical activity (MVPA) in bouts of ≥10 minutes for substantial health benefits. To what extent the same amount of MVPA accumulated in bouts versus sporadically reduces mortality risk remains unclear.
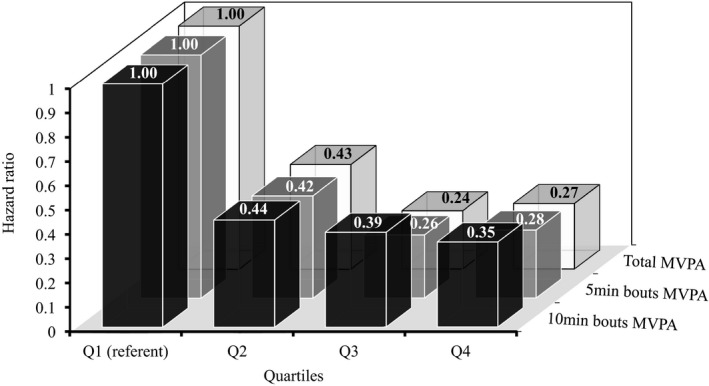
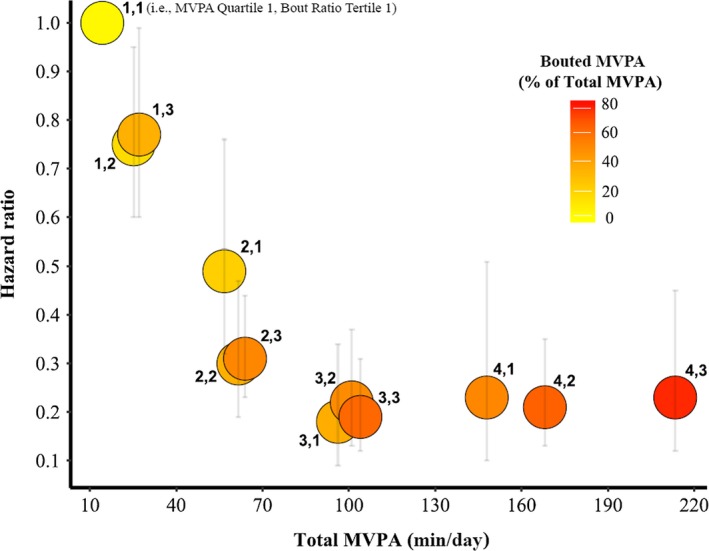
Methods and results: We analyzed data from the National Health and Nutrition Examination Survey 2003-2006 and death records available through 2011 (follow-up period of ≈6.6 years; 700 deaths) to examine the associations between objectively measured physical activity accumulated with and without a bout criteria and all-cause mortality in a representative sample of US adults 40 years and older (n=4840). Physical activity data were processed to generate minutes per day of total and bouted MVPA. Bouted MVPA was defined as MVPA accumulated in bouts of a minimum duration of either 5 or 10 minutes allowing for 1- to 2-minute interruptions. Hazard ratios for all-cause mortality associated with total and bouted MVPA were similar and ranged from 0.24 for the third quartile of total to 0.44 for the second quartile of 10-minute bouts. The examination of jointly classified quartiles of total MVPA and tertiles of proportion of bouted activity revealed that greater amounts of bouted MVPA did not result in additional risk reductions for mortality.
Conclusions: These results provide evidence that mortality risk reductions associated with MVPA are independent of how activity is accumulated and can impact the development of physical activity guidelines and inform clinical practice.
Keywords: National Health and Nutrition Examination Survey; accelerometer; activity bouts; adults; epidemiology; exercise.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
Comment in
-
Accumulation of Moderate-to-Vigorous Physical Activity and All-Cause Mortality.J Am Heart Assoc. 2018 Mar 22;7(6):e008929. doi: 10.1161/JAHA.118.008929. J Am Heart Assoc. 2018. PMID: 29567765 Free PMC article. No abstract available.
References
-
- US Department of Health and Human Services . Physical Activity Guidelines for Americans. 2008. Available at: http://www.health.gov/PAGuidelines. Accessed August 16, 2017.
-
- Pate RR, Pratt M, Blair SN, Haskell WL, Macera CA, Bouchard C, Buchner D, Ettinger W, Heath GW, King AC, Kriska A, Leon AS, Marcus BH, Morris J, Paffenberger RS, Patrick K, Pollock ML, Rippe JM, Sallis J, Wilmore JH. Physical activity and public health. A recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine. JAMA. 1995;273:402–407. - PubMed
-
- Physical Activity Guidelines Advisory Committee . Physical Activity Guidelines Advisory Committee Report, 2008. Washington, DC: US Department of Health and Human Services; 2008. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
