

The new allosteric inhibitor asciminib is susceptible to resistance mediated by ABCB1 and ABCG2 overexpression in vitro
- PMID: 29568367
- PMCID: PMC5862588
- DOI: 10.18632/oncotarget.24393
The new allosteric inhibitor asciminib is susceptible to resistance mediated by ABCB1 and ABCG2 overexpression in vitro
Abstract
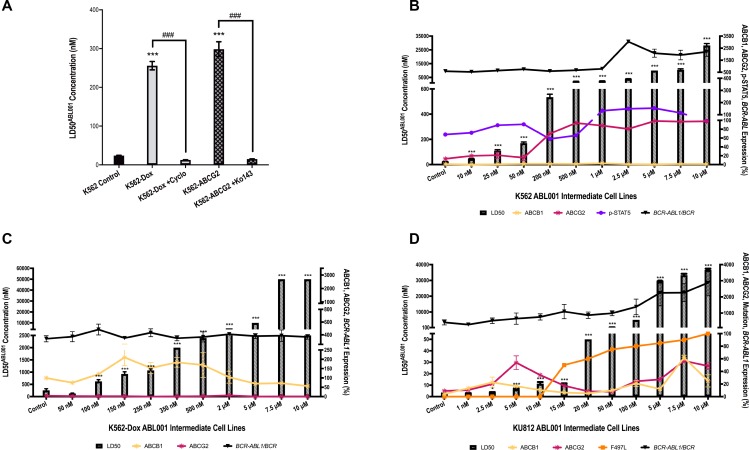
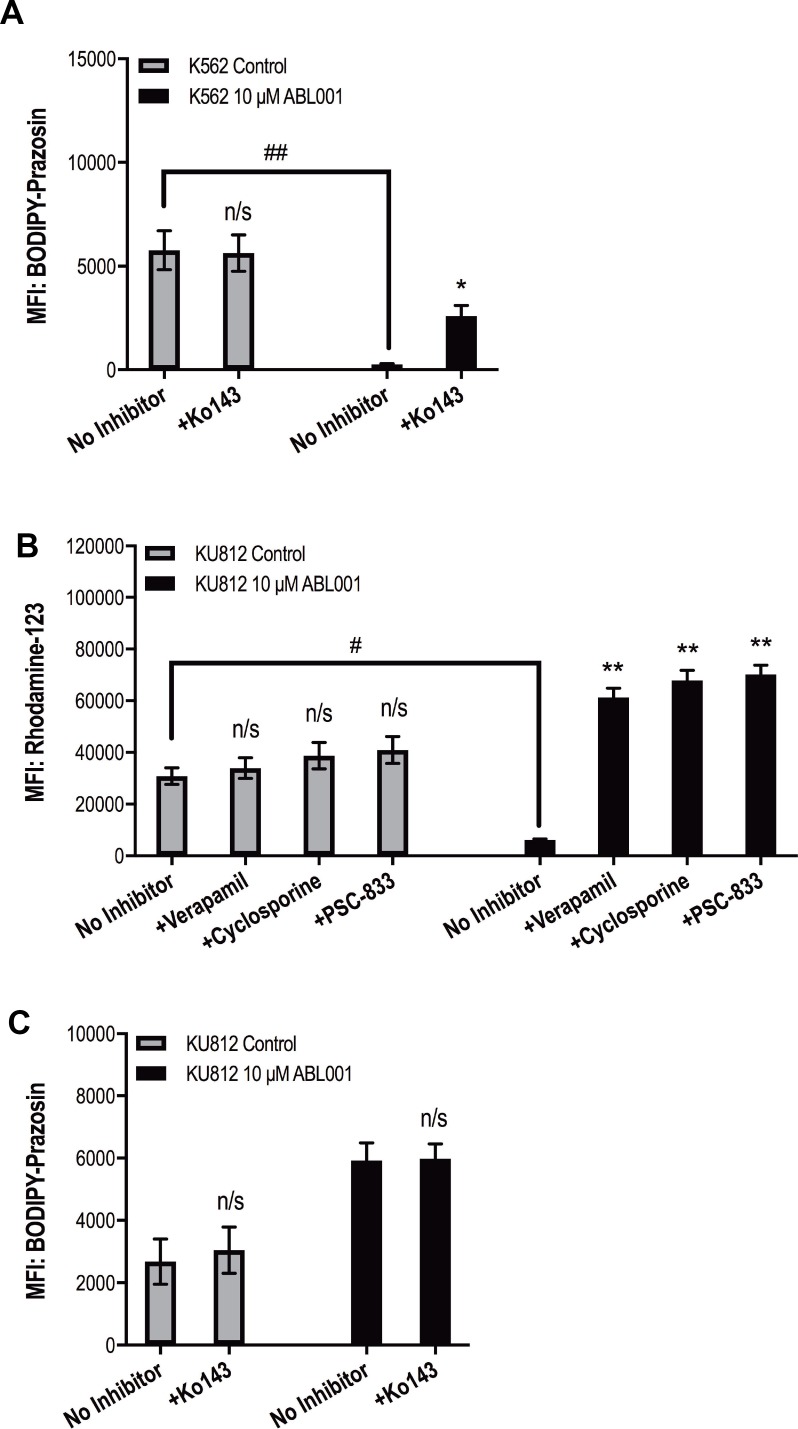
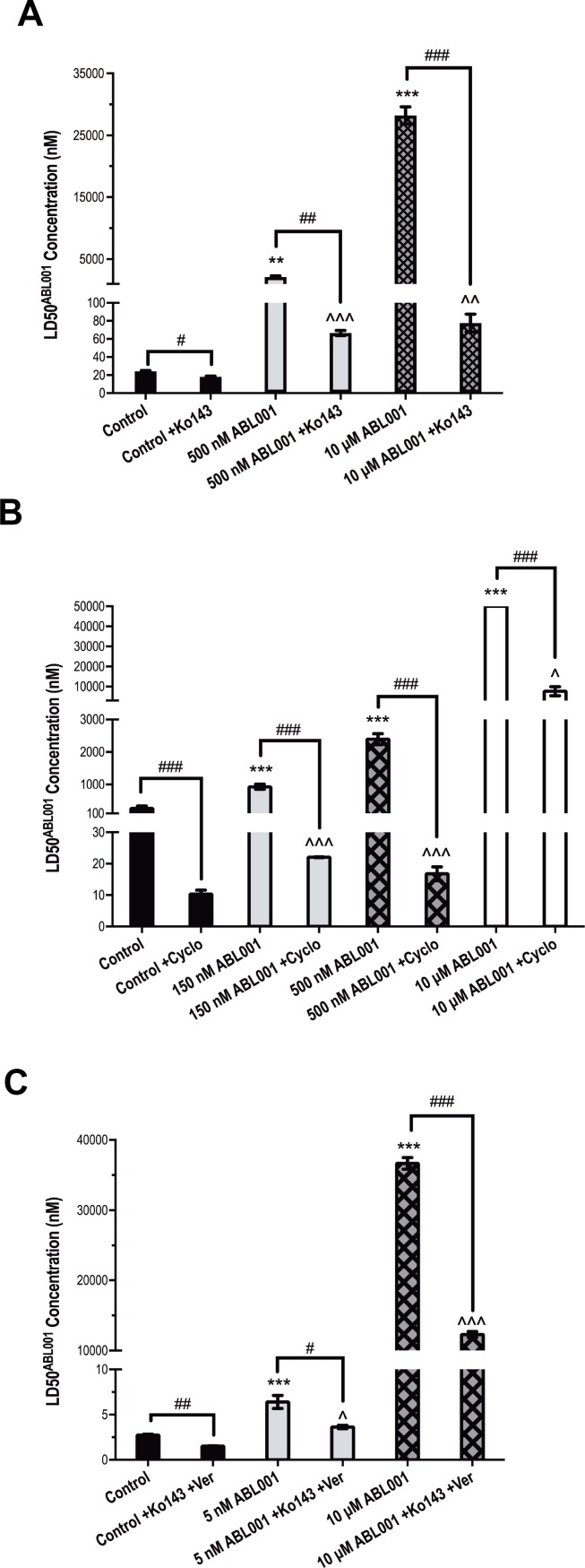
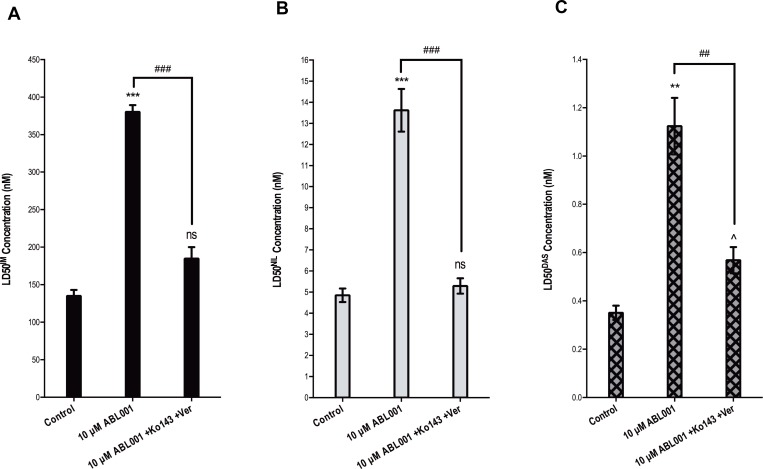
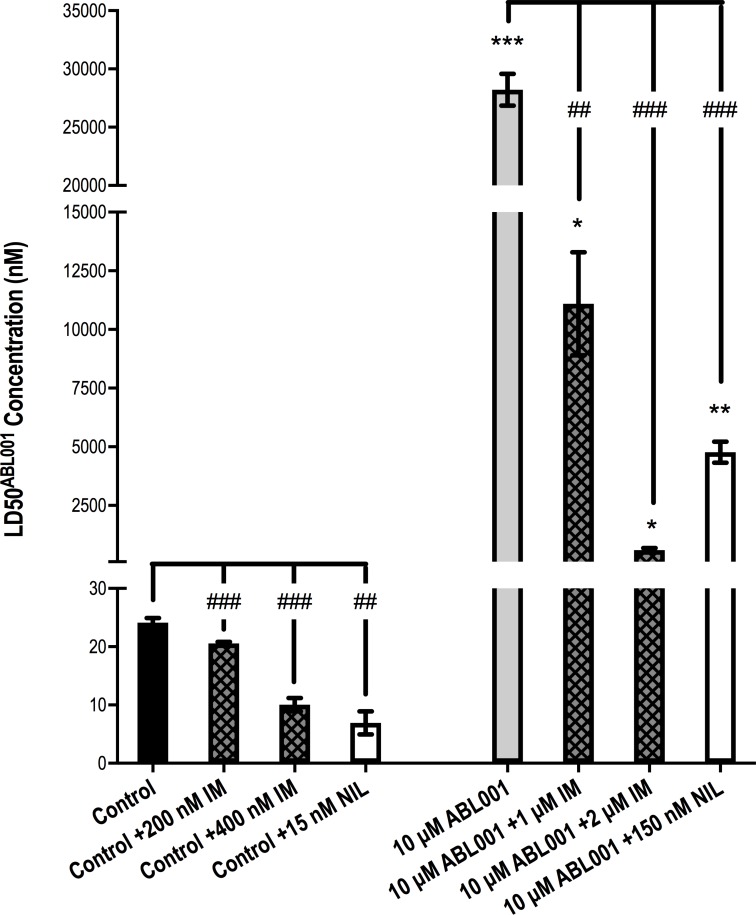
Asciminib (previously ABL001), which binds the myristate-binding pocket of the Bcr-Abl kinase domain, is in phase I clinical trials as monotherapy and in combination with imatinib, nilotinib and dasatinib for the treatment of patients with refractory CML or Ph+ ALL. Asciminib sensitivity was evaluated in asciminib naïve BCR-ABL1+ cell lines K562 (negligible ABCB1/ABCG2 expression), K562-Dox (ABCB1-overexpressing through doxorubicin exposure) and K562-ABCG2 (ABCG2 overexpression via transduction) with results demonstrating asciminib efflux by both ABCB1 and ABCG2 transporters. K562-Dox and K562-ABCG2 cells demonstrated increased LD50asciminib vs K562 control cells: 256 and 299 nM respectively vs 24 nM, p < 0.001. Sensitivity was completely restored with specific inhibitors cyclosporine (ABCB1) and Ko143 (ABCG2): K562-Dox LD50asciminib+cyclosporine = 13 nM, K562-ABCG2 LD50asciminib+Ko143 = 15 nM (p < 0.001). When asciminib resistance was modelled in vitro, ABCB1 and ABCG2 overexpression was integral in the development of asciminib resistance. In K562 asciminib-resistant cells, ABCG2 expression increased prior to BCR-ABL1 overexpression and remained high (up to 7.6-fold greater levels in resistant vs control cells, p < 0.001). K562-Dox asciminib-resistant cells had increased ABCB1 expression (2.1-fold vs control cells p = 0.0033). KU812 asciminib-resistant cells overexpressed ABCB1 (5.4-fold increase, p < 0.001) and ABCG2 (6-fold increase, p < 0.001) before emergence of a novel myristate-binding pocket mutation (F497L). In all three cell lines, asciminib resistance was reversible upon chemical inhibition of ABCB1, ABCG2 or both (p < 0.001). When K562 asciminib-resistant cells were treated with asciminib in combination with clinically achievable doses of either imatinib or nilotinib, reversal of the resistance phenotype was also observed (p < 0.01). Overexpression of efflux transporters will likely be an important pathway for asciminib resistance in the clinical setting. Given the lack of evidence for ABCG2-mediated transport of nilotinib or imatinib at clinically relevant concentrations, our data provide an additional rationale for using asciminib in combination with either TKI.
Keywords: ABCB1; ABCG2; ABL001; asciminib; resistance.
Conflict of interest statement
CONFLICTS OF INTEREST LNE and VAS have no conflict of interest to declare. DLW receives honoraria and research funds from Novartis Pharmaceuticals and is a member of Advisory Boards for Novartis. SB and TPH receive honoraria and research funds from Novartis Pharmaceuticals, BMS and Ariad and are members of Advisory Boards for Novartis, BMS and Ariad. However, Novartis, BMS and Ariad had no role in the design of the study, collection and analysis of data, nor the decision to publish.
Figures
References
-
- Druker BJ, Tamura S, Buchdunger E, Ohno S, Segal GM, Fanning S, Zimmermann J, Lydon NB. Effects of a selective inhibitor of the Abl tyrosine kinase on the growth of Bcr-Abl positive cells. Nat Med. 1996;2:561–6. - PubMed
-
- Druker BJ, Guilhot F, O’Brien SG, Gathmann I, Kantarjian H, Gattermann N, Deininger MW, Silver RT, Goldman JM, Stone RM, Cervantes F, Hochhaus A, Powell BL, et al. IRIS Investigators Five-year follow-up of patients receiving imatinib for chronic myeloid leukemia. N Engl J Med. 2006;355:2408–17. https://doi.org/10.1056/NEJMoa062867. - DOI - PubMed
-
- Hochhaus A, Saglio G, Larson RA, Kim DW, Etienne G, Rosti G, De Souza C, Kurokawa M, Kalaycio ME, Hoenekopp A, Fan X, Shou Y, Kantarjian HM, et al. Nilotinib is associated with a reduced incidence of BCR-ABL mutations vs imatinib in patients with newly diagnosed chronic myeloid leukemia in chronic phase. Blood. 2013;121:3703–8. https://doi.org/10.1182/blood-2012-04-423418. - DOI - PMC - PubMed
-
- Kantarjian H, Shah NP, Hochhaus A, Cortes J, Shah S, Ayala M, Moiraghi B, Shen Z, Mayer J, Pasquini R, Nakamae H, Huguet F, Boque C, et al. Dasatinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med. 2010;362:2260–70. https://doi.org/10.1056/NEJMoa1002315. - DOI - PubMed
-
- Giles FJ, le Coutre PD, Pinilla-Ibarz J, Larson RA, Gattermann N, Ottmann OG, Hochhaus A, Radich JP, Saglio G, Hughes TP, Martinelli G, Kim DW, Novick S, et al. Nilotinib in imatinib-resistant or imatinib-intolerant patients with chronic myeloid leukemia in chronic phase: 48-month follow-up results of a phase II study. Leukemia. 2013;27:107–12. https://doi.org/10.1038/leu.2012.181. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
