

Routine cranial computed tomography before lumbar puncture in HIV-positive adults presenting with seizures at Mitchells Plain Hospital, Cape Town
- PMID: 29568583
- PMCID: PMC5843182
- DOI: 10.4102/sajhivmed.v16i1.354
Routine cranial computed tomography before lumbar puncture in HIV-positive adults presenting with seizures at Mitchells Plain Hospital, Cape Town
Abstract
Background: Current international guidelines recommend that a cranial computed tomography (CT) be performed on all HIV-positive patients presenting with new onset seizures, before a lumbar puncture (LP) is performed. In the South African setting, however, this delay could be life threatening. The present study sought to measure the number of cranial CTs that contraindicate an LP and to predict which clinical signs and symptoms are likely to pose an increased risk from LP.
Methods: The study was performed at a district level hospital in Western Cape Province. Data were collected retrospectively from October 2013 to October 2014. Associations between categorical variables were analysed using Pearson's chi-squared test. Generalised linear regression was used to estimate prevalence ratios.
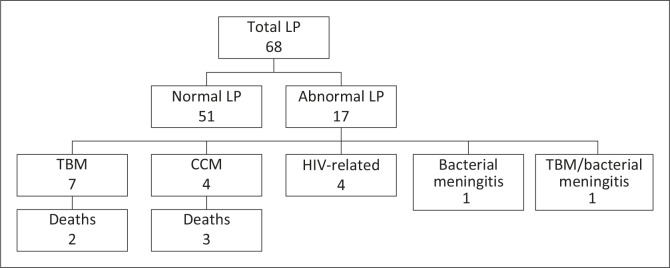
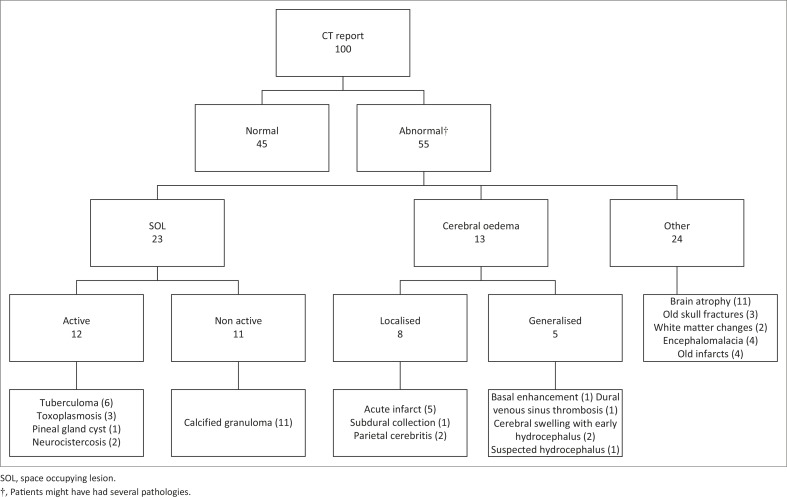
Results: One hundred out of 132 patients were studied. Brain shift contraindicated an LP in 5% of patients. Patients with brain shift presented with decreased level of consciousness, focal signs, headache and neck stiffness. Twenty-five per cent of patients had a space-occupying lesion (SOL) (defined as a discrete lesion that has a measurable volume) or cerebral oedema. Multivariate analysis showed a CD4 count <50 (p = 0.033) to be a statistically significant predictor of patients with SOL and cerebral oedema. Univariate analysis showed focal signs (p = 0.0001), neck stiffness (p = 0.05), vomiting (p = 0.018) and a Glascow Coma Scale (GCS) < 15 (p = 0.002) to be predictors of SOL and cerebral oedema.
Conclusion: HIV-positive patients with seizures have a high prevalence of SOL and cerebral oedema but the majority of them are safe for LP. Doctors can use clinical parameters to determine which patients can undergo immediate LP.
Conflict of interest statement
The authors declare that they have no financial or personal relationships which may have inappropriately influenced them in writing this article.
Figures
References
-
- Kellinghaus C, Enbring C, Kovac S, et al. Frequency of seizures and epilepsy in neurological HIV-infected patients. Seizure. 2007;17:27–33. http://dx.doi.org/10.1016/j.seizure.2007.05.017 - DOI - PubMed
-
- Gopal AK, Whitehouse JD, Simel DL, et al. Cranial computed tomography before lumbar puncture: A prospective clinical evaluation. Arch Intern Med. 1999;159:2681–2685. http://dx.doi.org/10.1001/archinte.159.22.2681 - DOI - PubMed
-
- Van Crevel H, Hijdra A, De Gans J.. Lumbar puncture and the risk of herniation: When should we perform CT? J Neurol. 2002;249:129–137. http://dx.doi.org/10.1007/PL00007855 - DOI - PubMed
-
- Hasbun R, Abrahams J, Jekel J, Quagliarello VJ.. Computed tomography of the head before lumbar puncture in adults with suspected meningitis. N Engl J Med. 2001;345:1727–1733. http://dx.doi.org/10.1056/NEJMoa010399 - DOI - PubMed
-
- Roytowski D, Figaji A.. Raised intracranial pressure: What it is and how to recognise it. CME. 2013;31:390–395.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials