

Stem-cell therapy in ST-segment elevation myocardial infarction with reduced ejection fraction: A multicenter, double-blind randomized trial
- PMID: 29569254
- PMCID: PMC6489870
- DOI: 10.1002/clc.22882
Stem-cell therapy in ST-segment elevation myocardial infarction with reduced ejection fraction: A multicenter, double-blind randomized trial
Abstract
Background: Left ventricular ejection fraction (LVEF) is a major determinant of long-term prognosis after ST-segment elevation myocardial infarction (STEMI). STEMI patients with reduced LVEF have a poor prognosis, despite successful reperfusion and the use of renin-angiotensin-aldosterone inhibitors.
Hypothesis: Intracoronary infusion of bone marrow-derived mononuclear cells (BMMC) may improve LVEF in STEMI patients successfully reperfused.
Methods: The main inclusion criteria for this double-blind, randomized, multicenter study were patient age 30 to 80 years, LVEF ≤50%, successful angioplasty of infarct-related artery, and regional dysfunction in the infarct-related area analyzed before cell injection. Cardiac magnetic resonance imaging was used to assess LVEF, left ventricular volumes, and infarct size at 7 to 9 days and 6 months post-myocardial infarction.
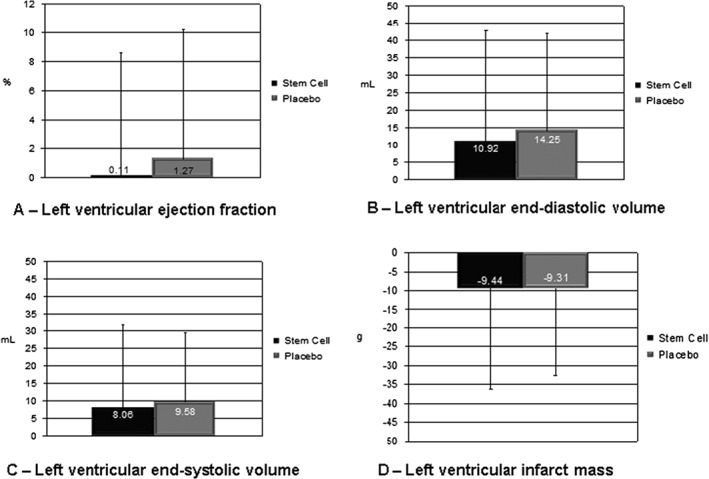
Results: One hundred and twenty-one patients were included (66 patients in the BMMC group and 55 patients in the placebo group). The primary endpoint, mean LVEF, was similar between both groups at baseline (44.63% ± 10.74% vs 42.23% ± 10.33%; P = 0.21) and at 6 months (44.74% ± 12.95 % vs 43.50 ± 12.43%; P = 0.59). The groups were also similar regarding the difference between baseline and 6 months (0.11% ± 8.5% vs 1.27% ± 8.93%; P = 0.46). Other parameters of left ventricular remodeling, such as systolic and diastolic volumes, as well as infarct size, were also similar between groups.
Conclusions: In this randomized, multicenter, double-blind trial, BMMC intracoronary infusion did not improve left ventricular remodeling or decrease infarct size.
Keywords: Acute Coronary Syndrome; Cardiomyopathy; Ischemic Heart Disease; Myocardial Infarction; Stem Cell Therapy.
© 2018 Wiley Periodicals, Inc.
Conflict of interest statement
The authors declare no potential conflicts of interest.
Figures


References
-
- Global Burden of Disease 2013 Mortality and Causes of Death Collaborators . Global, regional, and national age‐sex specific all‐cause and cause‐specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385:117–171. - PMC - PubMed
-
- Volpi A, De Vita C, Franzosi MG, et al; The Ad Hoc Working Group of the Gruppo Italiano per lo Studio della Sopravvivenza nell'Infarto Miocardico (GISSI)‐2 Database . Determinants of 6‐month mortality in survivors of myocardial infarction after thrombolysis: results of the GISSI‐2 database. Circulation. 1993;88:416–429. - PubMed
-
- Richards AM, Nicholls MG, Espiner EA, et al. B‐type natriuretic peptides and ejection fraction for prognosis after myocardial infarction. Circulation. 2003;107:2786–2792. - PubMed
-
- Dagres N, Hindricks G. Risk stratification after myocardial infarction: is left ventricular ejection fraction enough to prevent sudden cardiac death? Eur Heart J. 2013;34:1964–1971. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
