

Assessment of recording bias in pregnancy studies using health care databases: An application to neurologic conditions
- PMID: 29569366
- PMCID: PMC5980700
- DOI: 10.1111/ppe.12459
Assessment of recording bias in pregnancy studies using health care databases: An application to neurologic conditions
Abstract
Background: Pre-existing conditions are imperfectly recorded in health care databases. We assessed whether pre-existing neurologic conditions (epilepsy, multiple sclerosis [MS]) were differentially recorded in the presence of major obstetric outcomes (Caesarean delivery, preterm delivery, preeclampsia) in delivery records. We also evaluated the impact of differential recording on measures of frequency and association between the conditions and outcomes.
Methods: The 2011-2014 Truven Health MarketScan® Commercial Claims Dataset was used to identify pregnancies. We calculated the relative recording of epilepsy and MS at delivery hospitalization compared with a 270-day pre-delivery window both overall and by the presence of major obstetric outcomes. We estimated risk ratios for the association between epilepsy and MS with the outcomes for each ascertainment window.
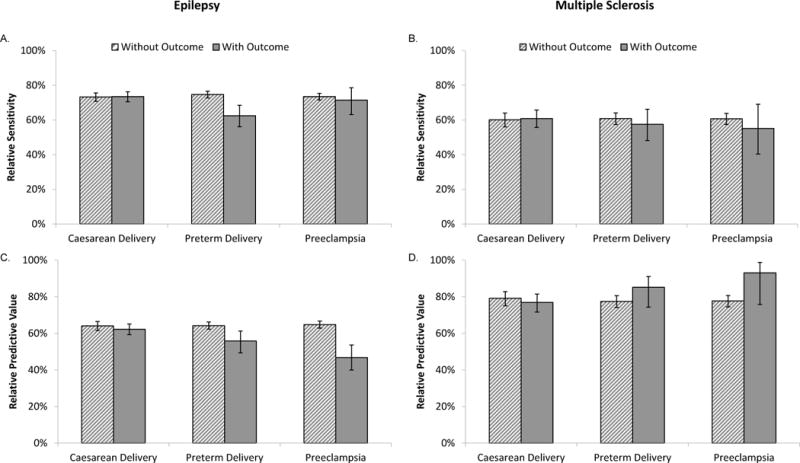
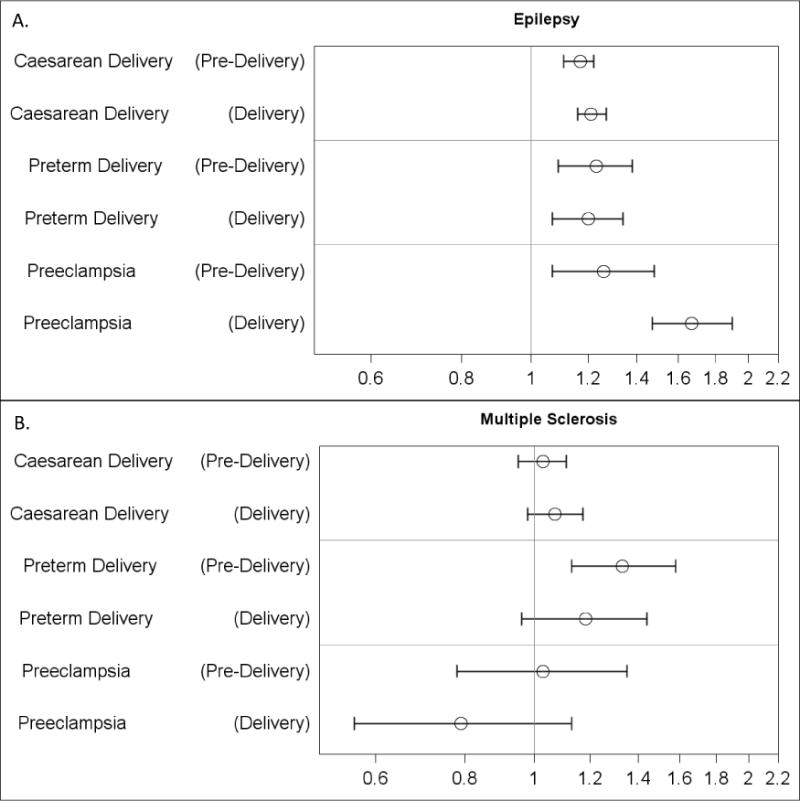
Results: We identified 909 065 pregnancies in women continuously enrolled from 270-days before the delivery date. Of women with epilepsy identified in the pre-delivery window, 73% had the condition coded at delivery. For MS, the proportion was 60%. MS recording at delivery did not vary by obstetric outcomes, however, delivery-coded epilepsy was less likely confirmed in the pre-delivery window in the presence of preeclampsia. Generally, the period of ascertainment did not meaningfully impact risk ratios, however, the risk ratio for preeclampsia associated with epilepsy was 1.67 (95% CI 1.47, 1.90) when epilepsy was ascertained at delivery and 1.26 (95% CI 1.07, 1.48) when epilepsy was ascertained in the pre-delivery window (heterogeneity, P = .007).
Conclusions: Ascertainment of epilepsy and MS in delivery hospitalization records underestimated prevalence. However, the window of recording generally did not impact risk ratio estimates of associations with obstetric outcomes.
Keywords: administrative claims; bias (epidemiology); epilepsy; health care; multiple sclerosis; pregnancy.
© 2018 John Wiley & Sons Ltd.
Figures
Comment in
-
Making the best use of data not created for research.Paediatr Perinat Epidemiol. 2018 May;32(3):287-289. doi: 10.1111/ppe.12466. Epub 2018 Mar 25. Paediatr Perinat Epidemiol. 2018. PMID: 29575116 Free PMC article. No abstract available.
References
-
- Drews CD, Kraus JF, Greenland S. Recall bias in a case-control study of sudden infant death syndrome. Int J Epidemiol. 1990;19(2):405–411. - PubMed
-
- Yasmeen S, Romano PS, Schembri ME, et al. Accuracy of obstetric diagnoses and procedures in hospital discharge data. Am J Obstet Gynecol. 2006;194(4):992–1001. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
