

Digoxin use and lower risk of 30-day all-cause readmission in older patients with heart failure and reduced ejection fraction receiving β-blockers
- PMID: 29569405
- PMCID: PMC6489941
- DOI: 10.1002/clc.22889
Digoxin use and lower risk of 30-day all-cause readmission in older patients with heart failure and reduced ejection fraction receiving β-blockers
Abstract
Background: Digoxin use has been associated with a lower risk of 30-day all-cause admission and readmission in patients with heart failure and reduced ejection fraction (HFrEF).
Hypothesis: Digoxin use will be associated with improved outcomes in patients with HFrEF receiving β-blockers.
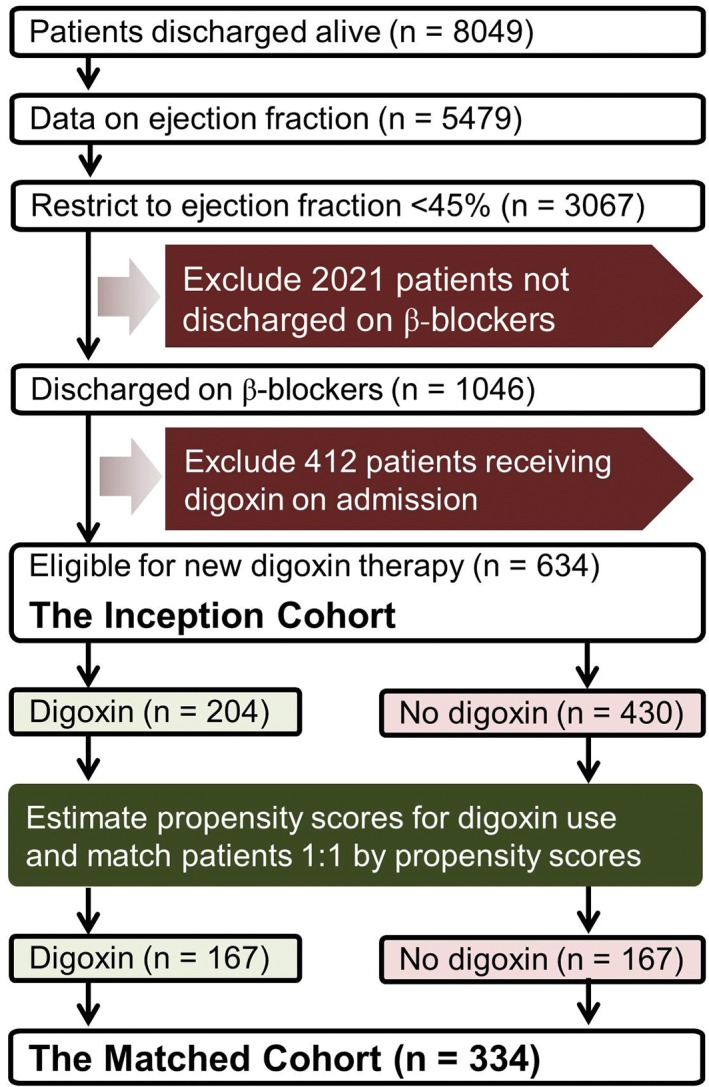
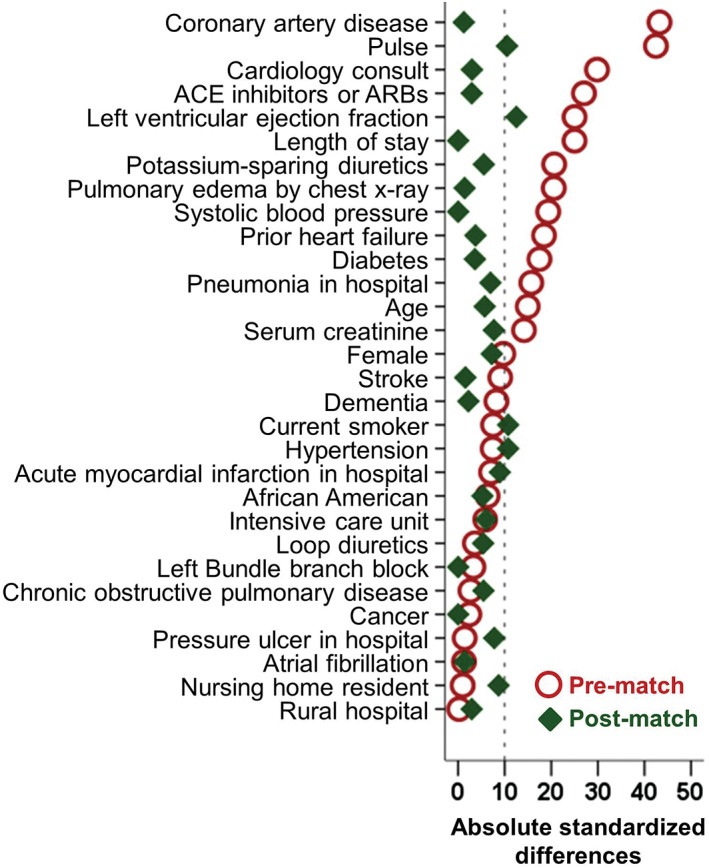
Methods: Of the 3076 hospitalized Medicare beneficiaries with HFrEF (EF <45%), 1046 received a discharge prescription for β-blockers, of which 634 were not on digoxin. Of the 634, 204 received a new discharge prescription for digoxin. Propensity scores for digoxin use, estimated for each of the 634 patients, were used to assemble a matched cohort of 167 pairs of patients receiving and not receiving digoxin, balanced on 30 baseline characteristics. Matched patients (n = 334) had a mean age of 74 years and were 46% female and 30% African American.
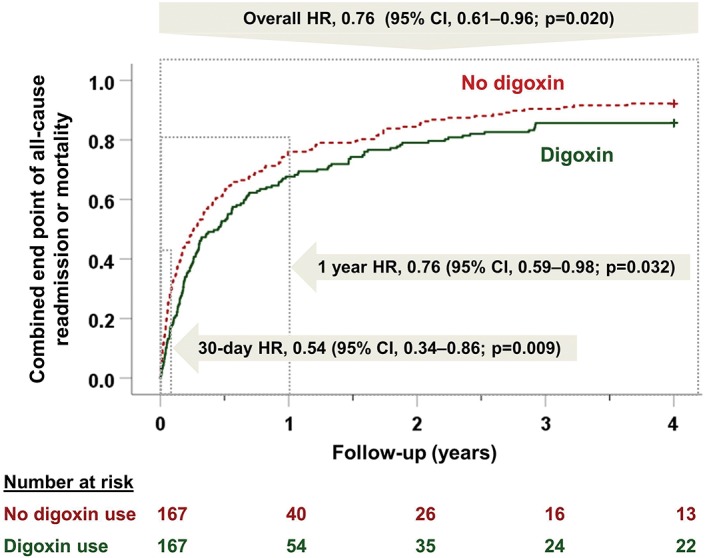
Results: 30-day all-cause readmission occurred in 15% and 27% of those receiving and not receiving digoxin, respectively (hazard ratio [HR]: 0.51, 95% confidence interval [CI]: 0.31-0.83, P = 0.007). This beneficial association persisted during 4 years of follow-up (HR: 0.72, 95% CI: 0.57-0.92, P = 0.008). Digoxin use was also associated with a lower risk of the combined endpoint of all-cause readmission or all-cause mortality at 30 days (HR: 0.54, 95% CI: 0.34-0.86, P = 0.009) and at 4 years (HR: 0.76, 95% CI: 0.61-0.96, P = 0.020).
Conclusions: In hospitalized patients with HFrEF receiving β-blockers, digoxin use was associated with a lower risk of 30-day all-cause readmission but not mortality, which persisted during longer follow-up.
Keywords: Digoxin; Heart Failure; Hospital Readmission; β-Blockers.
© 2018 Wiley Periodicals, Inc.
Conflict of interest statement
The authors declare no potential conflicts of interest.
Figures
References
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee‐for‐service program [published correction appears in N Engl J Med. 2011;364:1582]. N Engl J Med. 2009;360:1418–1428. - PubMed
-
- Digitalis Investigation Group Investigators . The effect of digoxin on mortality and morbidity in patients with heart failure. N Engl J Med. 1997;336:525–533. - PubMed
-
- Packer M, Bristow MR, Cohn JN, et al; US Carvedilol Heart Failure Study Group . The effect of carvedilol on morbidity and mortality in patients with chronic heart failure. N Engl J Med. 1996;334:1349–1355. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
