

Immediate effects and outcome of in-utero pulmonary valvuloplasty in fetuses with pulmonary atresia with intact ventricular septum or critical pulmonary stenosis
- PMID: 29569770
- PMCID: PMC6100104
- DOI: 10.1002/uog.19047
Immediate effects and outcome of in-utero pulmonary valvuloplasty in fetuses with pulmonary atresia with intact ventricular septum or critical pulmonary stenosis
Abstract
Objective: To assess the immediate effects of fetal pulmonary valvuloplasty on right ventricular (RV) size and function as well as in-utero RV growth and postnatal outcome.
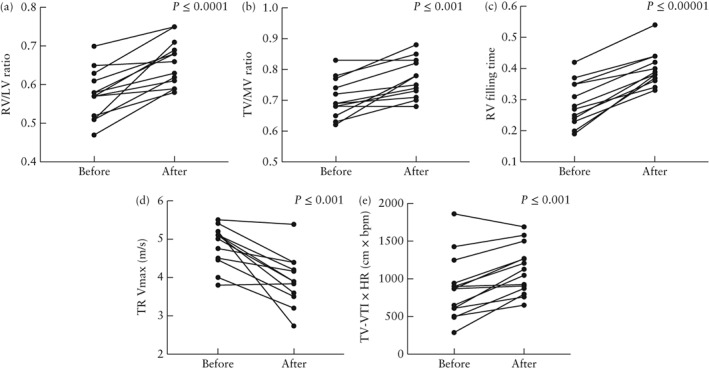
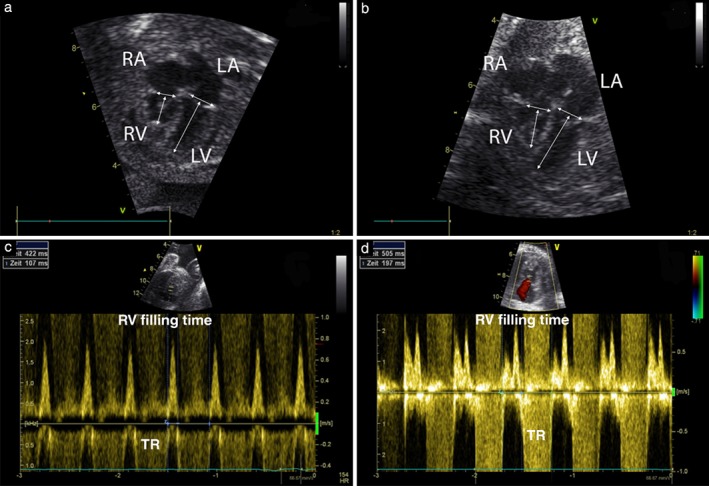
Methods: Patients with pulmonary atresia with intact ventricular septum (PAIVS) or critical pulmonary stenosis (CPS) who underwent fetal pulmonary valvuloplasty at our center between October 2000 and July 2017 were included. Echocardiographic data obtained before and after the procedure were analyzed retrospectively (median interval after intervention, 1 (range, 1-3) days) for ventricular and valvular dimensions and ratios, RV filling time (duration of tricuspid valve (TV) inflow/cardiac cycle length), TV velocity time integral (TV-VTI) × heart rate (HR) and tricuspid regurgitation (TR) velocity. Longitudinal data were collected from only those fetuses followed up in our center. Outcome was assessed using the scoring system as described by Roman et al. for non-biventricular outcome.
Results: Thirty-five pulmonary valvuloplasties were performed in our institution on 23 fetuses with PAIVS (n = 15) or CPS (n = 8). Median gestational age at intervention was 28 + 4 (range, 23 + 6 to 32 + 1) weeks. No fetal death occurred. Immediately after successful intervention, RV/left ventricular length (RV/LV) ratio (P ≤ 0.0001), TV/mitral valve annular diameter (TV/MV) ratio (P ≤ 0.001), RV filling time (P ≤ 0.00001) and TV-VTI × HR (P ≤ 0.001) increased significantly and TR velocity (P ≤ 0.001) decreased significantly. In fetuses followed longitudinally to delivery (n = 5), RV/LV and TV/MV ratios improved further or remained constant until birth. Fetuses with unsuccessful intervention (n = 2) became univentricular, all others had either a biventricular (n = 15), one-and-a-half ventricular (n = 3) or still undetermined (n = 3) outcome. Five of nine fetuses with a predicted non-biventricular outcome, in which the procedure was successful, became biventricular, while two of nine had an undetermined circulation.
Conclusion: In selected fetuses with PAIVS or CPS, in-utero pulmonary valvuloplasty led immediately to larger RV caused by reduced afterload and increased filling, thus improving the likelihood of biventricular outcome even in fetuses with a predicted non-biventricular circulation. © 2018 The Authors. Ultrasound in Obstetrics & Gynecology published by John Wiley & Sons Ltd on behalf of the International Society of Ultrasound in Obstetrics and Gynecology.
Keywords: congenital heart disease; fetal cardiac intervention; fetal pulmonary valvuloplasty; pulmonary atresia with intact septum.
© 2018 The Authors. Ultrasound in Obstetrics & Gynecology published by John Wiley & Sons Ltd on behalf of the International Society of Ultrasound in Obstetrics and Gynecology.
Figures

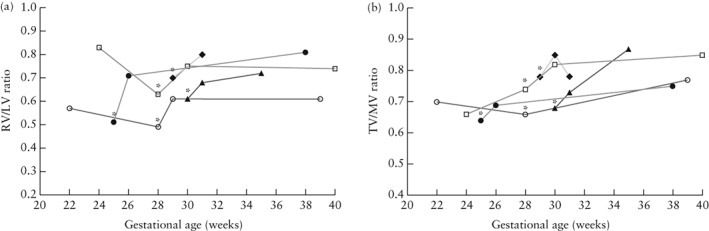
 , Patient 6;
, Patient 6;  , Patient 11;
, Patient 11;  , Patient 18;
, Patient 18;  , Patient 19;
, Patient 19;  , Patient 21.
, Patient 21.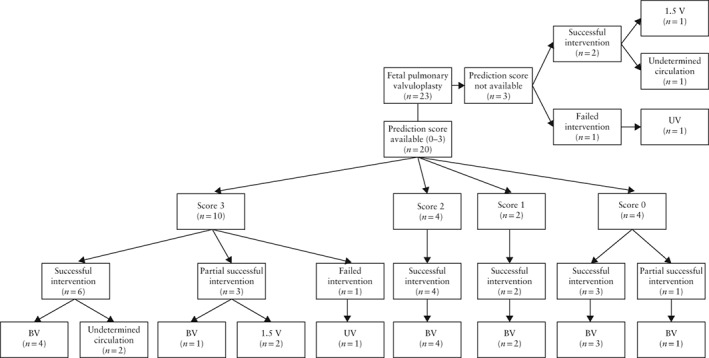
Similar articles
-
Fetal Pulmonary Valvuloplasty in Fetuses with Right Ventricular Outflow Tract Obstructive Disease: Experience and Outcome of the First Five Cases in China.Pediatr Cardiol. 2021 Feb;42(2):340-348. doi: 10.1007/s00246-020-02488-8. Epub 2020 Oct 22. Pediatr Cardiol. 2021. PMID: 33090241
-
[Prenatal interventional therapy in two cases with critical pulmonary stenosis or pulmonary atresia with intact ventricular septum].Zhonghua Er Ke Za Zhi. 2018 Jun 2;56(6):445-450. doi: 10.3760/cma.j.issn.0578-1310.2018.06.008. Zhonghua Er Ke Za Zhi. 2018. PMID: 29886608 Chinese.
-
Biventricular impact of mild to moderate fetal pulmonary valve stenosis.Ultrasound Obstet Gynecol. 2018 Mar;51(3):349-356. doi: 10.1002/uog.17456. Ultrasound Obstet Gynecol. 2018. PMID: 28295792
-
Prediction of postnatal circulation in pulmonary atresia/critical stenosis with intact ventricular septum: systematic review and external validation of models.Ultrasound Obstet Gynecol. 2023 Jul;62(1):14-22. doi: 10.1002/uog.26176. Epub 2023 Jun 5. Ultrasound Obstet Gynecol. 2023. PMID: 36776132
-
Fetal Echocardiographic Predictors of Postnatal Surgical Strategies in Critical Pulmonary Stenosis or Atresia with Intact Ventricular Septum: A Meta-Analysis.Fetal Diagn Ther. 2022;49(5-6):225-234. doi: 10.1159/000525718. Epub 2022 Jul 6. Fetal Diagn Ther. 2022. PMID: 35793649
Cited by
-
Natural history of pulmonary atresia with intact ventricular septum (PAIVS) and critical pulmonary stenosis (CPS) and prediction of outcome.Arch Gynecol Obstet. 2021 Jul;304(1):81-90. doi: 10.1007/s00404-020-05929-0. Epub 2021 Feb 14. Arch Gynecol Obstet. 2021. PMID: 33585987 Free PMC article.
-
Integrative Perinatal Management Enhanced the Advantage of Prenatal Diagnosis on Critical Pulmonary Valve Stenosis: An Observational Preliminary Study.Front Pediatr. 2020 Dec 21;8:572238. doi: 10.3389/fped.2020.572238. eCollection 2020. Front Pediatr. 2020. PMID: 33409260 Free PMC article.
-
Mending a broken heart: In vitro, in vivo and in silico models of congenital heart disease.Dis Model Mech. 2021 Mar 28;14(3):dmm047522. doi: 10.1242/dmm.047522. Dis Model Mech. 2021. PMID: 33787508 Free PMC article. Review.
-
Fetal Cardiac Interventions-Polish Experience from "Zero" to the Third World Largest Program.J Clin Med. 2020 Sep 7;9(9):2888. doi: 10.3390/jcm9092888. J Clin Med. 2020. PMID: 32906670 Free PMC article.
-
Prenatal diagnosis of congenital heart defects: echocardiography.Transl Pediatr. 2021 Aug;10(8):2210-2224. doi: 10.21037/tp-20-164. Transl Pediatr. 2021. PMID: 34584892 Free PMC article. Review.
References
-
- Dyamenahalli U, McCrindle BW, McDonald C, Trivedi KR, Smallhorn JF, Benson LN, Coles J, Williams WG, Freedom RM. Pulmonary atresia with intact ventricular septum: management of, and outcomes for, a cohort of 210 consecutive patients. Cardiol Young 2004; 14: 299–308. - PubMed
-
- Rice MJ, McDonald RW, Reller MD. Progressive pulmonary stenosis in the fetus: two case reports. Am J Perinatol 1993; 10: 424–427. - PubMed
-
- Todros T, Presbitero P, Gaglioti P, Demarie D. Pulmonary stenosis with intact ventricular septum: documentation of development of the lesion echocardiographically during fetal life. Int J Cardiol 1988; 19: 355–62. - PubMed
-
- Daubeney PE, Sharland GK, Cook AC, Keeton BR, Anderson RH, Webber SA. Pulmonary atresia with intact ventricular septum: impact of fetal echocardiography on incidence at birth and postnatal outcome. UK and Eire Collaborative Study of Pulmonary Atresia with Intact Ventricular Septum. Circulation 1998; 98: 562–566. - PubMed
-
- Salvin JW, McElhinney DB, Colan SD, Gauvreau K, del Nido PJ, Jenkins KJ, Lock JE, Tworetzky W. Fetal tricuspid valve size and growth as predictors of outcome in pulmonary atresia with intact ventricular septum. Pediatrics 2006; 118: e415–420. - PubMed
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
