

Immunogenicity of type 2 monovalent oral and inactivated poliovirus vaccines for type 2 poliovirus outbreak response: an open-label, randomised controlled trial
- PMID: 29571817
- PMCID: PMC10495755
- DOI: 10.1016/S1473-3099(18)30113-0
Immunogenicity of type 2 monovalent oral and inactivated poliovirus vaccines for type 2 poliovirus outbreak response: an open-label, randomised controlled trial
Abstract
Background: Monovalent type 2 oral poliovirus vaccine (mOPV2) and inactivated poliovirus vaccine (IPV) are used to respond to type 2 poliovirus outbreaks. We aimed to assess the effect of two mOPV2 doses on the type 2 immune response by varying the time interval between mOPV2 doses and IPV co-administration with mOPV2.
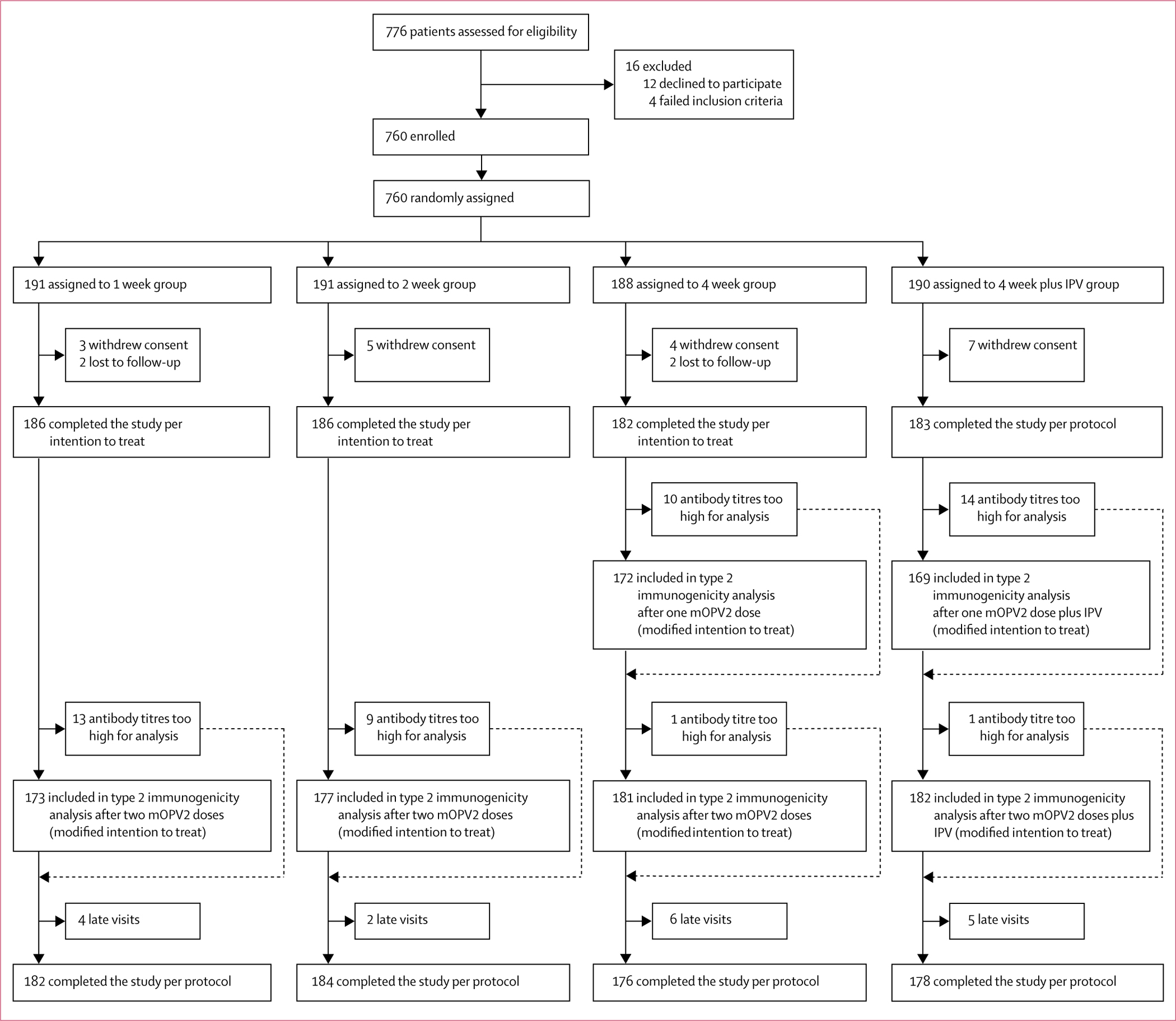
Methods: We did a randomised, controlled, parallel, open-label, non-inferiority, inequality trial at two study clinics in Dhaka, Bangladesh. Healthy infants aged 6 weeks (42-48 days) at enrolment were randomly assigned (1:1:1:1) to receive two mOPV2 doses (each dose consisting of two drops [0·1 mL in total] of about 105 50% cell culture infectious dose of type 2 Sabin strain) at intervals of 1 week, 2 weeks, 4 weeks (standard or control group), or 4 weeks with IPV (0·5 mL of type 1 [Mahoney, 40 D-antigen units], type 2 [MEF-1, 8 D-antigen units], and type 3 [Saukett, 32 D-antigen units]) administered intramuscularly with the first mOPV2 dose. We used block randomisation, randomly selecting blocks of sizes four, eight, 12, or 16 stratified by study sites. We concealed randomisation assignment from staff managing participants in opaque, sequentially numbered, sealed envelopes. Parents and clinic staff were unmasked to assignment after the randomisation envelope was opened. Laboratory staff analysing sera were masked to assignment, but investigators analysing data and assessing outcomes were not. The primary outcome was type 2 immune response measured 4 weeks after mOPV2 administration. The primary modified intention-to-treat analysis included participants with testable serum samples before and after vaccination. A non-inferiority margin of 10% and p=0·05 (one-tailed) was used. This trial is registered at ClinicalTrials.gov, number NCT02643368, and is closed to accrual.
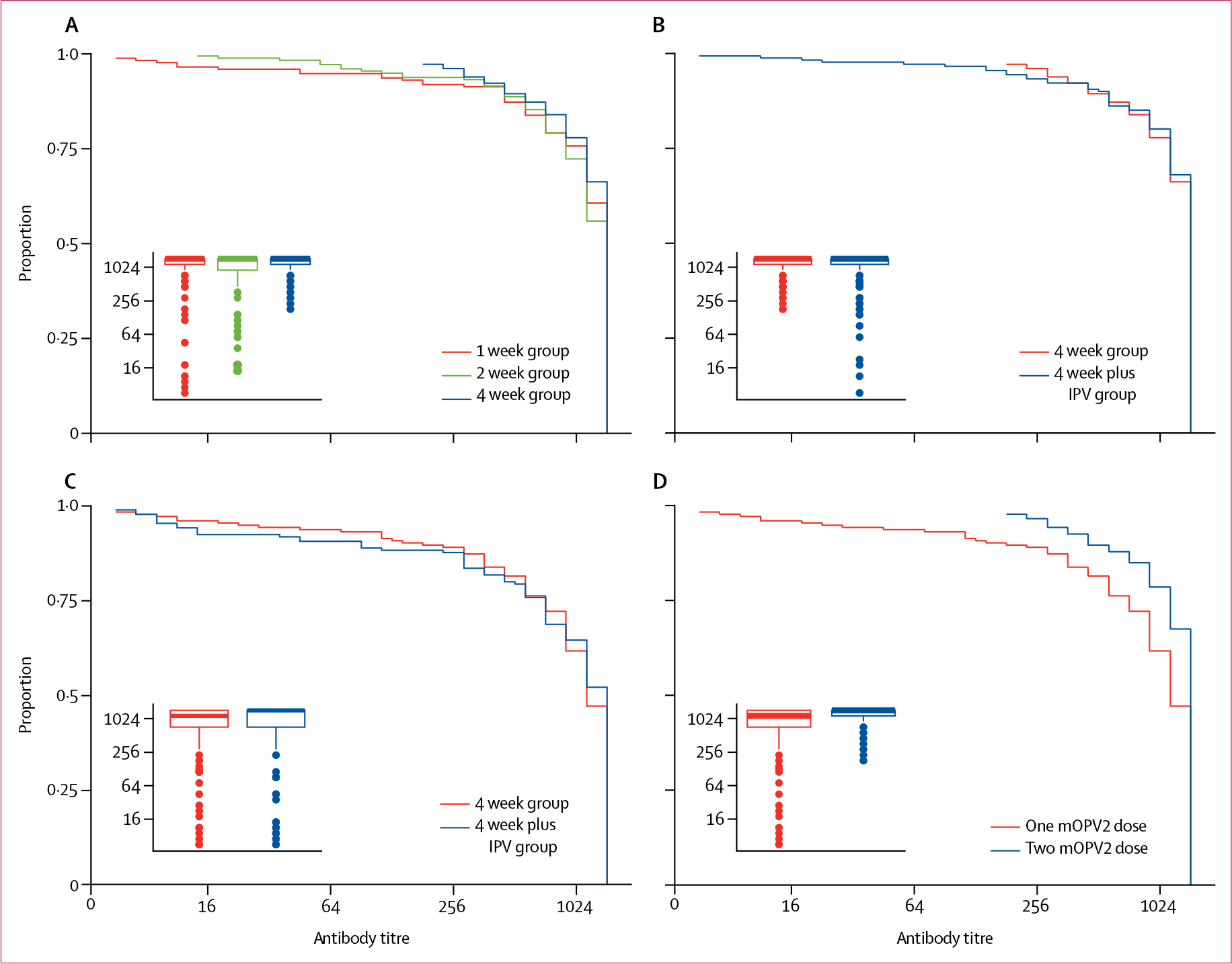
Findings: Between Dec 7, 2015, and Jan 5, 2016, we randomly assigned 760 infants to receive two mOPV2 doses at intervals of 1 week (n=191), 2 weeks (n=191), 4 weeks (n=188), or 4 weeks plus IPV (n=190). Immune responses after two mOPV2 doses were observed in 161 (93%) of 173 infants with testable serum samples in the 1 week group, 169 (96%) of 177 in the 2 week group, and 176 (97%) of 181 in the 4 week group. 1 week and 2 week intervals between two mOPV2 doses were non-inferior to 4 week intervals because the lower bound of the absolute differences in the percentage of immune responses were greater than -10% (-4·2% [90% CI -7·9 to -0·4] in the 1 week group and -1·8% [-5·0 to 1·5] in the 2 week group vs the 4 week group). The immune response elicited by two mOPV2 doses 4 weeks apart was not different when IPV was added to the first dose (176 [97%] of 182 infants with IPV vs 176 [97%] of 181 without IPV; p=1·0). During the trial, two serious adverse events (pneumonia; one [1%] of 186 patients in the 1 week group and one [1%] of 182 in the 4 week group) and no deaths were reported; the adverse events were not attributed to the vaccines.
Interpretation: Administration of mOPV2 at short intervals does not interfere with its immunogenicity. The addition of IPV to the first mOPV2 dose did not improve poliovirus type 2 immune response.
Funding: US Centers for Disease Control and Prevention.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests
MSO reports grants from Bill & Melinda Gates Foundation and royalties to institution for licensing of enterovirus and parechovirus strains for redistribution as reagents or controls from Zeptometrix outside the submitted work. All other authors declare no competing interests.
Figures
Comment in
-
Eradicating polio with a vaccine we must stop using.Lancet Infect Dis. 2018 Jun;18(6):590-591. doi: 10.1016/S1473-3099(18)30174-9. Epub 2018 Mar 20. Lancet Infect Dis. 2018. PMID: 29571818 No abstract available.
References
-
- Dowdle WR, Cochi SL. Global eradication of poliovirus: history and rationale. In: Semler BL, Wimmer E, eds. Molecular biology of picornaviruses. Washington, DC: ASM Press, 2002: 473–80.
-
- Sutter RW, Kew OM, Cochi SL, Aylward RB. Poliovirus vaccine—live. In: Plotkin SA, Orenstein WA, Offit PA, eds. Vaccines 6th edn. China: Elsevier, 2013: 598–645.
-
- Caceres VM, Sutter RW. Sabin monovalent oral polio vaccines: review of past experiences and their potential use after polio eradication. Clin Infect Dis 2001; 33: 531–41. - PubMed
-
- Birmingham ME, Aylward RB, Cochi SL, Hull HF. National immunization days: state of the art. J Infect Dis 1997; 175 (suppl 1): S183–88. - PubMed
-
- Cochi SL, Linkins RW. The final phase of polio eradication: new vaccines and complex choices. J Infect Dis 2012; 205: 169–71. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
