

Impact of temporary methotrexate discontinuation for 2 weeks on immunogenicity of seasonal influenza vaccination in patients with rheumatoid arthritis: a randomised clinical trial
- PMID: 29572291
- PMCID: PMC5965360
- DOI: 10.1136/annrheumdis-2018-213222
Impact of temporary methotrexate discontinuation for 2 weeks on immunogenicity of seasonal influenza vaccination in patients with rheumatoid arthritis: a randomised clinical trial
Abstract
Objective: To determine whether a 2-week methotrexate (MTX) discontinuation after vaccination improves the efficacy of seasonal influenza vaccination in patients with rheumatoid arthritis (RA).
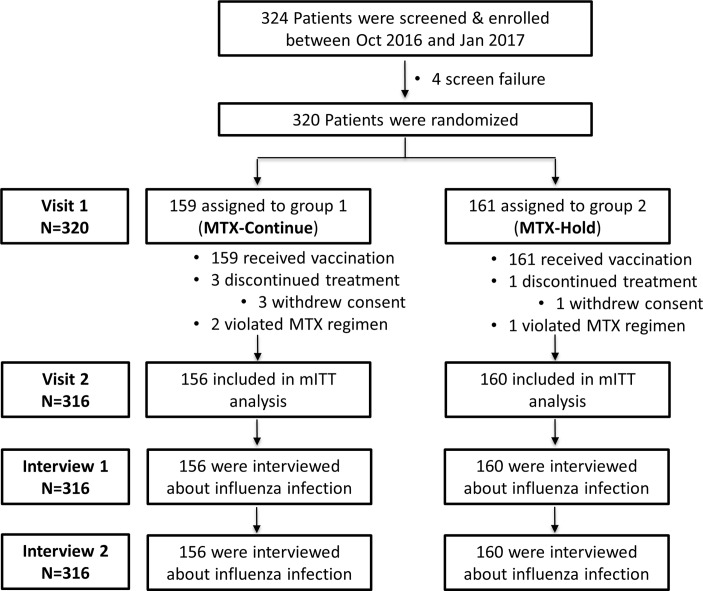
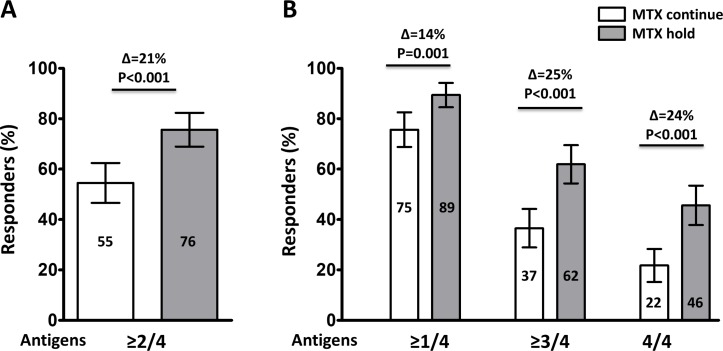
Methods: In this prospective randomised parallel-group multicentre study, patients with RA on stable dose of MTX were randomly assigned at a ratio of 1:1 to continue MTX or to hold MTX for 2 weeks after 2016-2017 quadrivalent seasonal influenza vaccine containing H1N1, H3N2, B-Yamagata and B-Victoria. The primary outcome was frequency of satisfactory vaccine response, defined as greater than or equal to fourfold increase of haemagglutination inhibition (HI) antibody titre at 4 weeks after vaccination against ≥2 of four vaccine strains. Secondary endpoints included seroprotection (ie, HI titre ≥1:40) rate, fold change in antibody titres.
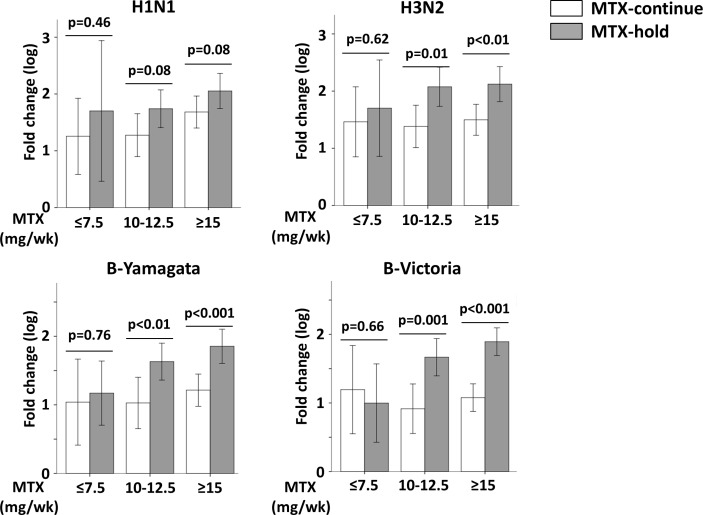
Results: The modified intention-to-treat population included 156 patients in the MTX-continue group and 160 patients in the MTX-hold group. More patients in MTX-hold group achieved satisfactory vaccine response than the MTX-continue group (75.5% vs 54.5%, p<0.001). Seroprotection rate was higher in the MTX-hold group than the MTX-continue group for all four antigens (H1N1: difference 10.7%, 95% CI 2.0% to 19.3%; H3N2: difference 15.9%, 95% CI 5.9% to 26.0%; B-Yamagata: difference13.7%, 95% CI 5.2% to 22.4%; B-Victoria: difference 14.7%, 95% CI 4.5% to 25.0%). The MTX-hold group showed higher fold increase in their antibody titres against all four influenza antigens (all p<0.05). Change in disease activity was similar between groups.
Conclusions: A temporary MTX discontinuation for 2 weeks after vaccination improves the immunogenicity of seasonal influenza vaccination in patients with RA without increasing RA disease activity.
Trial registration: NCT02897011.
Keywords: discontinuation; influenza; methotrexate; rheumatoid arthritis; vaccination.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: EBL has acted as a consultant to Pfizer and received research grants from Green Cross Corporation and Hanmi Pharm.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
