

Impact of a commercial order entry system on prescribing errors amenable to computerised decision support in the hospital setting: a prospective pre-post study
- PMID: 29572298
- PMCID: PMC6109251
- DOI: 10.1136/bmjqs-2017-007135
Impact of a commercial order entry system on prescribing errors amenable to computerised decision support in the hospital setting: a prospective pre-post study
Abstract
Background: In this UK study, we investigated the impact of computerised physician order entry (CPOE) and clinical decision support (CDS) implementation on the rate of 78 high-risk prescribing errors amenable to CDS.
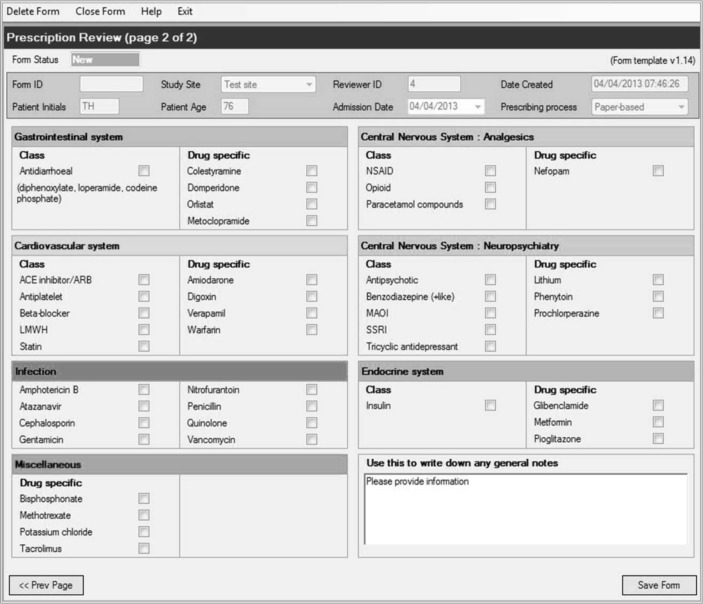
Methods: We conducted a preintervention/postintervention study in three acute hospitals in England. A predefined list of prescribing errors was incorporated into an audit tool. At each site, approximately 4000 prescriptions were reviewed both pre-CPOE and 6 months post-CPOE implementation. The number of opportunities for error and the number of errors that occurred were collated. Error rates were then calculated and compared between periods, as well as by the level of CDS.
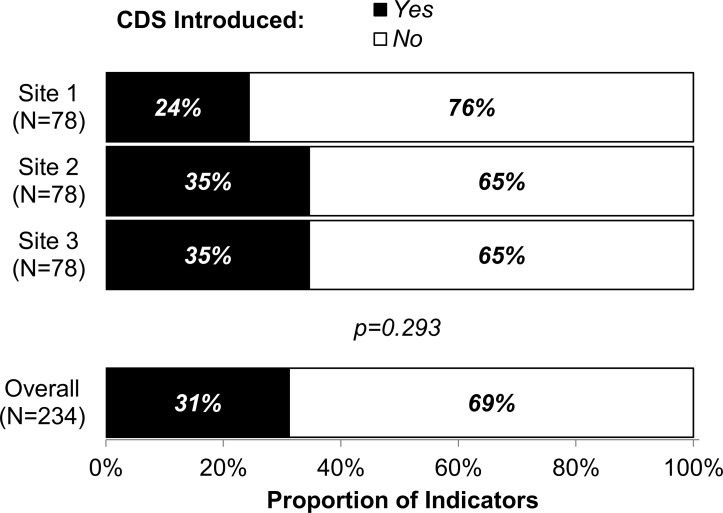
Results: The prescriptions of 1244 patients were audited pre-CPOE and 1178 post-CPOE implementation. A total of 28 526 prescriptions were reviewed, with 21 138 opportunities for error identified based on 78 defined errors. Across the three sites, for those prescriptions where opportunities for error were identified, the error rate was found to reduce significantly post-CPOE implementation, from 5.0% to 4.0% (P<0.001). CDS implementation by error type was found to differ significantly between sites, ranging from 0% to 88% across clinical contraindication, dose/frequency, drug interactions and other error types (P<0.001). Overall, 43/78 (55%) of the errors had some degree of CDS implemented in at least one of the hospitals.
Conclusions: Implementation of CPOE with CDS was associated with clinically important reductions in the rate of high-risk prescribing errors. Given the pre-post design, these findings however need to be interpreted with caution. The occurrence of errors was found to be highly dependent on the level of restriction of CDS presented to the prescriber, with the effect that different configurations of the same CPOE system can produce very different results.
Keywords: decision support, clinical; decision support, computerized; hospital medicine; medication safety.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical