

Prevalence, Causes, and Predictors of 30-Day Readmissions Following Hospitalization With Acute Myocardial Infarction Complicated By Cardiogenic Shock: Findings From the 2013-2014 National Readmissions Database
- PMID: 29572325
- PMCID: PMC5907572
- DOI: 10.1161/JAHA.117.008235
Prevalence, Causes, and Predictors of 30-Day Readmissions Following Hospitalization With Acute Myocardial Infarction Complicated By Cardiogenic Shock: Findings From the 2013-2014 National Readmissions Database
Abstract
Background: Prior studies have shown that survivors of acute myocardial infarction (AMI) complicated by cardiogenic shock are likely to have increased risk of readmissions in the early post-discharge period. However, the contemporary prevalence, reasons, and predictors of 30-day readmissions are not well known.
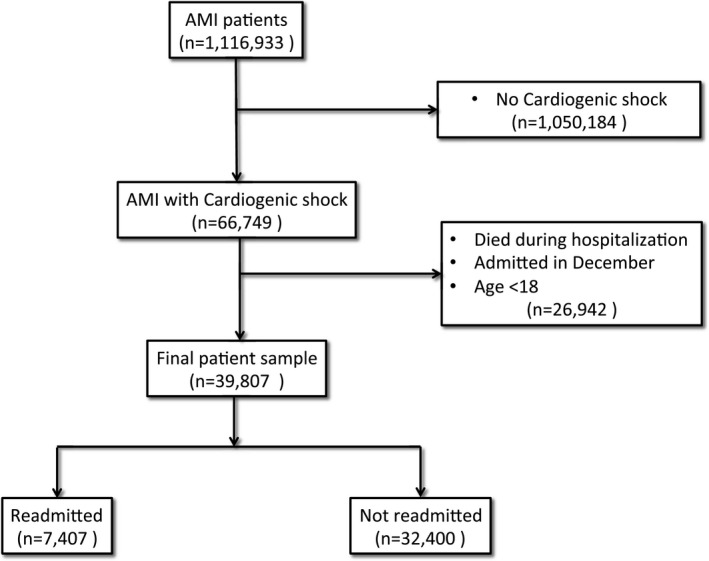
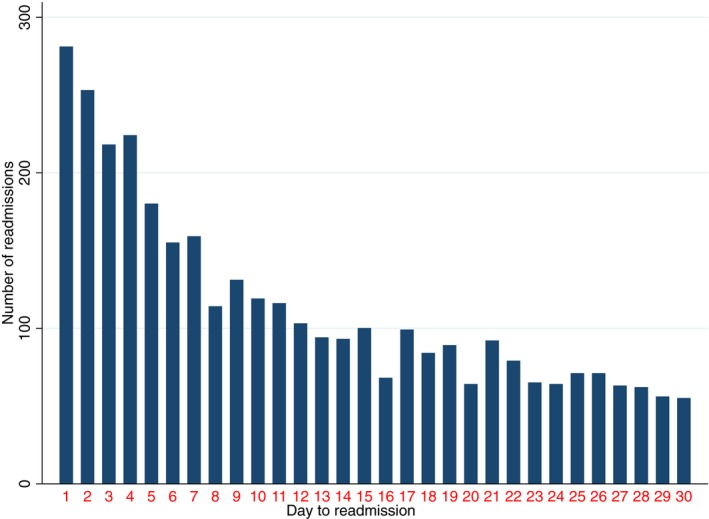
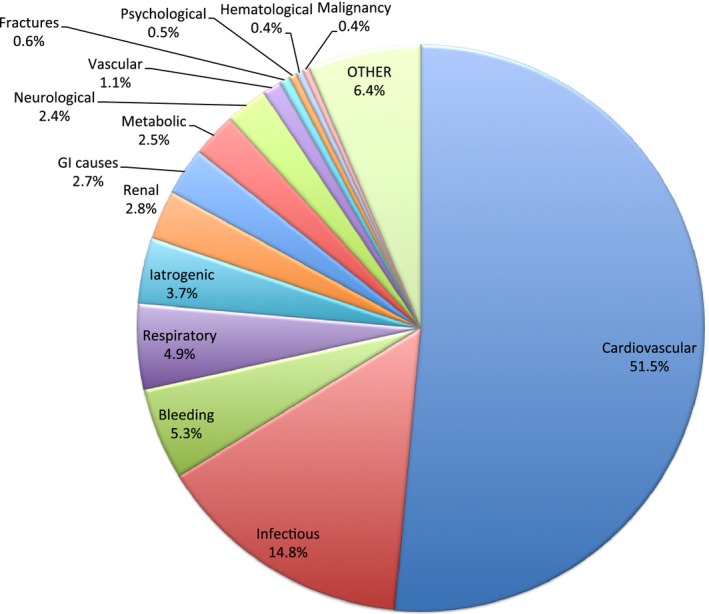
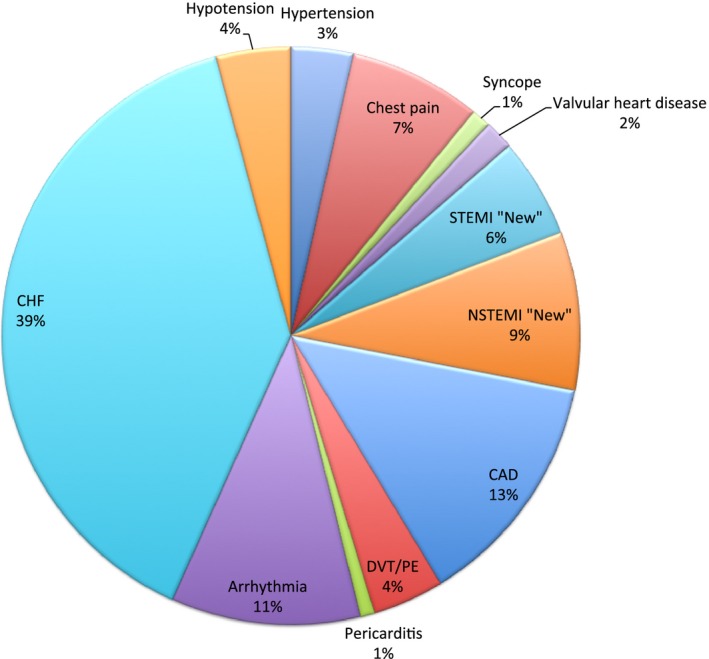
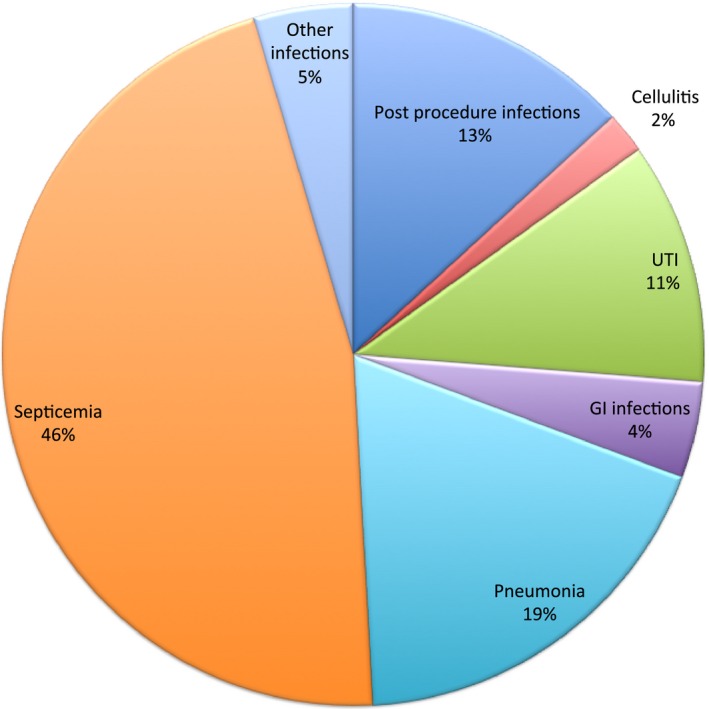
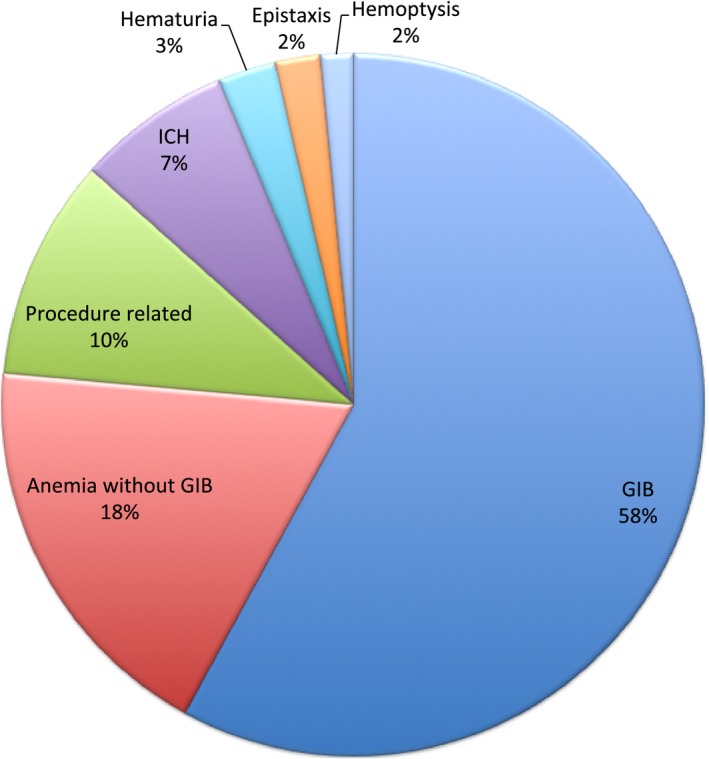
Methods and results: Hospitalizations for a primary diagnosis of AMI complicated by cardiogenic shock, and discharged alive, were identified in the 2013 and 2014 Nationwide Readmissions Databases. Prevalence and reasons for 30-day unplanned readmissions were investigated. A hierarchical logistic regression model was used to identify independent predictors of 30-day readmissions. Among 1 116 933 patient hospitalizations with AMI, 39 807 (3.6%) had cardiogenic shock and were discharged alive. Their 30-day readmission rate was 18.6%, with a median time for readmission 10 days post discharge. Predictors of readmission included: non-ST-segment elevation myocardial infarction, female sex, low-income status, nonprivate insurance, chronic renal failure, long-term ventricular assist device or intra-aortic balloon placement, and tachyarrhythmia. The majority of readmissions were attributable to cardiac-related causes (52%); heart failure being the most frequent cardiac cause (39% of all cardiac causes). Noncardiac-related readmissions included infections (14.9%), bleeding (5.3%), and respiratory causes (4.9%). The median cost per readmission was $9473 US dollars ($5037-20 199).
Conclusions: Among survivors of AMI complicated by cardiogenic shock who were discharged from hospital, almost 1 in 5 are readmitted at 30 days, mainly because of cardiac reasons such as heart failure and new AMI. The risk of readmission was associated with certain baseline patient/hospital characteristics.
Keywords: cardiogenic shock; heart failure; myocardial infarction; readmission.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Holmes DR Jr, Bates ER, Kleiman NS, Sadowski Z, Horgan JH, Morris DC, Califf RM, Berger PB, Topol EJ. Contemporary reperfusion therapy for cardiogenic shock: the GUSTO‐I trial experience. The GUSTO‐I Investigators. Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries. J Am Coll Cardiol. 1995;26:668–674. - PubMed
-
- Hochman JS, Buller CE, Sleeper LA, Boland J, Dzavik V, Sanborn TA, Godfrey E, White HD, Lim J, LeJemtel T. Cardiogenic shock complicating acute myocardial infarction–etiologies, management and outcome: a report from the SHOCK Trial Registry. SHould we emergently revascularize Occluded Coronaries for cardiogenic shocK? J Am Coll Cardiol. 2000;36:1063–1070. - PubMed
-
- Babaev A, Frederick PD, Pasta DJ, Every N, Sichrovsky T, Hochman JS. Trends in management and outcomes of patients with acute myocardial infarction complicated by cardiogenic shock. JAMA. 2005;294:448–454. - PubMed
-
- Anderson ML, Peterson ED, Peng SA, Wang TY, Ohman EM, Bhatt DL, Saucedo JF, Roe MT. Differences in the profile, treatment, and prognosis of patients with cardiogenic shock by myocardial infarction classification: a report from NCDR. Circ Cardiovasc Qual Outcomes. 2013;6:708–715. - PubMed
-
- Wayangankar SA, Bangalore S, McCoy LA, Jneid H, Latif F, Karrowni W, Charitakis K, Feldman DN, Dakik HA, Mauri L, Peterson ED, Messenger J, Roe M, Mukherjee D, Klein A. Temporal trends and outcomes of patients undergoing percutaneous coronary interventions for cardiogenic shock in the setting of acute myocardial infarction: a report from the CathPCI Registry. JACC Cardiovasc Interv. 2016;9:341–351. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
