

Neuroblastoma: clinical and biological approach to risk stratification and treatment
- PMID: 29572647
- PMCID: PMC5918153
- DOI: 10.1007/s00441-018-2821-2
Neuroblastoma: clinical and biological approach to risk stratification and treatment
Abstract
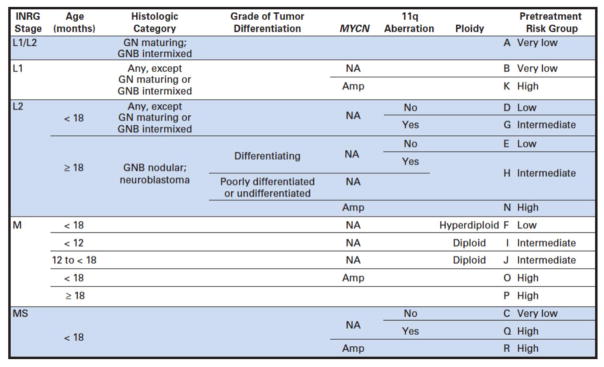
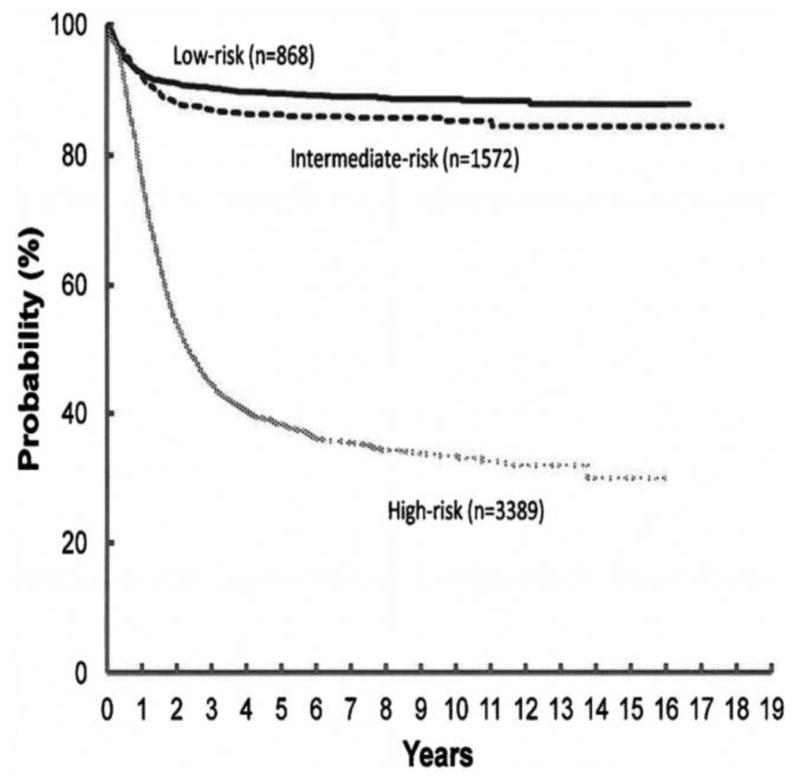
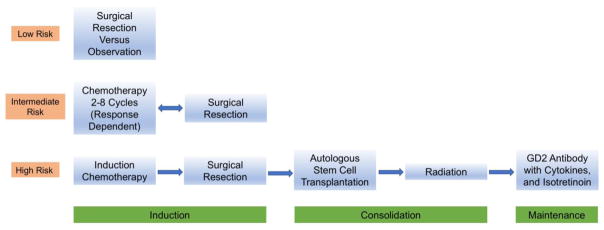
Neuroblastoma is the most common extra-cranial solid tumor of childhood and the most common in the first year of life. It is a unique malignancy in that infants often present with either localized or metastatic disease that can spontaneously regress without intervention while older children can succumb to the disease after months to years of arduous therapy. Given this wide range of outcomes, the International Neuroblastoma Risk Group was created to stratify patients based on presenting characteristics and tumor biology in order to guide intensity of treatment strategies. The goal has been to decrease therapy for low-risk patients to avoid long-term complications while augmenting and targeting therapies for high-risk patients to improve overall survival. The international risk stratification depends on age, stage, histology, MYCN gene amplification status, tumor cell ploidy and segmental chromosomal abnormalities. Treatment for asymptomatic low-risk patients with an estimated survival of > 98% is often observation or surgical resection alone, whereas intermediate-risk patients with an estimated survival of > 90% require moderate doses of response-adjusted chemotherapy along with resection. High-risk patients undergo multiple cycles of combination chemotherapy before surgery, followed by consolidation with myeloablative autologous hematopoietic stem cell transplantation and local radiation and finally immunotherapy with differentiation therapy as maintenance phase. With this approach, outcome for patients with neuroblastoma has improved, as the field continues to expand efforts in more targeted therapies for high-risk patients.
Keywords: Clinical presentation; Neuroblastoma; Pediatric oncology; Risk classification; Treatment.
Conflict of interest statement
Figures
References
-
- Adkins ES, Sawin R, Gerbing RB, London WB, Matthay KK, Haase GM. Efficacy of complete resection for high-risk neuroblastoma: a Children's Cancer Group study. J Pediatr Surg. 2004;39:931–936. - PubMed
-
- Ambros PF, Ambros IM, Brodeur GM, Haber M, Khan J, Nakagawara A, Schleiermacher G, Speleman F, Spitz R, London WB, Cohn SL, Pearson AD, Maris JM. International consensus for neuroblastoma molecular diagnostics: report from the International Neuroblastoma Risk Group (INRG) Biology Committee. Br J Cancer. 2009;100:1471–1482. - PMC - PubMed
-
- Amoroso L, Erminio G, Makin G, Pearson AD, Brock P, Valteau-Couanet D, Castel V, Pasquet M, Laureys G, Thomas C, Luksch R, Ladenstein R, Haupt R, Garaventa A, Group S. Topotecan-Vincristine-Doxorubicin in Stage 4 High Risk Neuroblastoma Patients Failing to Achieve a Complete Metastatic Response to Rapid COJEC - a SIOPEN Study. Cancer Res Treat 2017 - PMC - PubMed
-
- Antunes NL, Khakoo Y, Matthay KK, Seeger RC, Stram DO, Gerstner E, Abrey LE, Dalmau J. Antineuronal antibodies in patients with neuroblastoma and paraneoplastic opsoclonus-myoclonus. J Pediatr Hematol Oncol. 2000;22:315–320. - PubMed
-
- Attiyeh EF, London WB, Mosse YP, Wang Q, Winter C, Khazi D, McGrady PW, Seeger RC, Look AT, Shimada H, Brodeur GM, Cohn SL, Matthay KK, Maris JM Children's Oncology G. Chromosome 1p and 11q deletions and outcome in neuroblastoma. N Engl J Med. 2005;353:2243–2253. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
