

Detection, characterization, and enrollment of donors of Ebola convalescent plasma in Sierra Leone
- PMID: 29572862
- PMCID: PMC5947131
- DOI: 10.1111/trf.14580
Detection, characterization, and enrollment of donors of Ebola convalescent plasma in Sierra Leone
Abstract
Background: Passive therapy with convalescent plasma provides an early opportunity to intervene in Ebola virus disease (EVD). Methods for field screening and selection of potential donors and quantifying plasma antibody are needed.
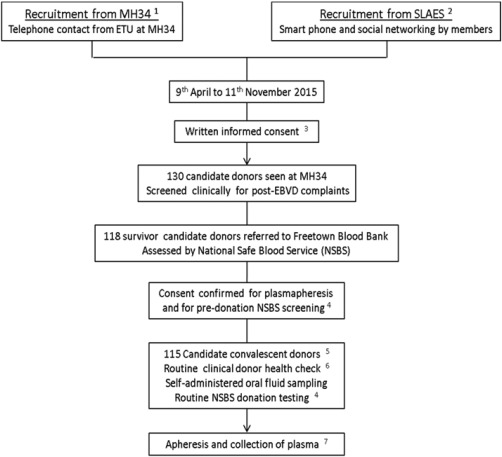
Study design and methods: Recombinant Ebola virus glycoprotein (EBOV GP) was formatted into immunoglobulin G-capture, competitive, and double-antigen bridging enzyme immunoassays (EIAs). EVD survivors in Freetown, Sierra Leone, were recruited as potential plasma donors and assessed locally using sera alone and/or paired sera and oral fluids (ORFs). Uninfected controls comprised unexposed Gambians and communities in Western Area, Sierra Leone. Antibody neutralization in selected sera was measured retrospectively in a pseudotype virus assay.
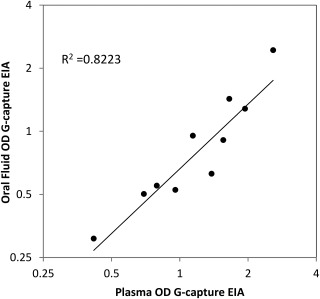
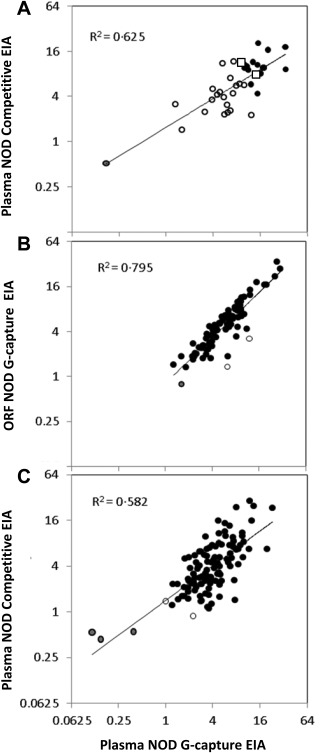
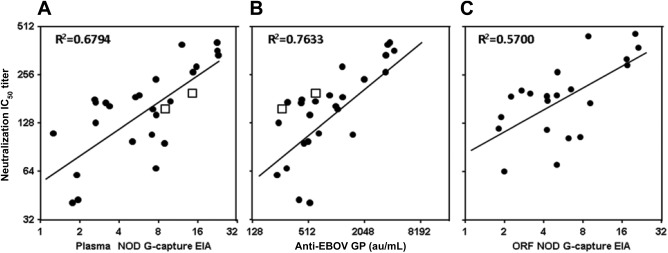
Results: A total of 115 potential donors were considered for enrollment: 110 plasma samples were concordantly reactive in the three EIAs; three were concordantly unreactive and two were reactive in two of three EIAs (98.2% agreement; 95% confidence interval [CI], 93.9%-99.8%). In 88 donors with paired ORF and plasma, G-capture EIA reactivity correlated well in the two analytes (R2 = 0.795). Plasma and ORF from 44 Gambians were unreactive. ORF samples from 338 of 339 unexposed Western Area community controls were unreactive (specificity, 99.7%; 95% CI, 98.4%-99.7%); ORF samples from 113 of 116 Kerry Town EVD survivors were reactive (sensitivity, 97.4%; 95% CI, 92.5%-99.5%). Strong reactivity in G-capture and/or competitive EIAs identified donors with high plasma EBOV GP antibody levels in the double-antigen bridging assay, correlating with high levels of neutralizing antibody.
Conclusions: In-field testing can qualify convalescent donors for providing high-titer antibody.
© 2018 The Authors Transfusion published by Wiley Periodicals, Inc. on behalf of AABB.
Conflict of interest statement
The authors have disclosed no conflicts of interest.
Figures

References
-
- Mupapa K, Massamba M, Kibadi K, et al. Treatment of Ebola hemorrhagic fever with blood transfusions from convalescent patients. International Scientific and Technical Committee . J Infect Dis 1999;179 Suppl 1 :S18‐23. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
