

Individualized immunoglobulin therapy in chronic immune-mediated peripheral neuropathies
- PMID: 29573033
- PMCID: PMC6033159
- DOI: 10.1111/jns.12262
Individualized immunoglobulin therapy in chronic immune-mediated peripheral neuropathies
Abstract
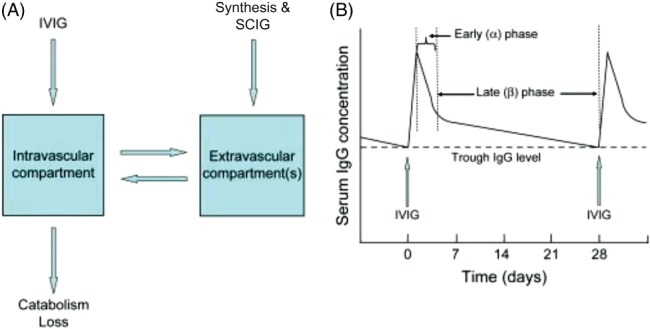
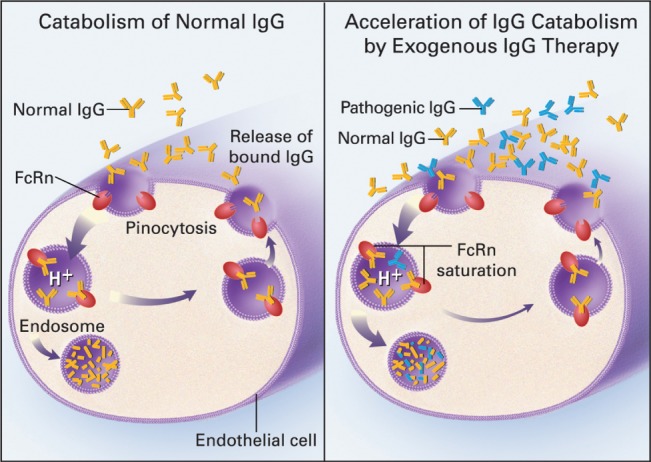
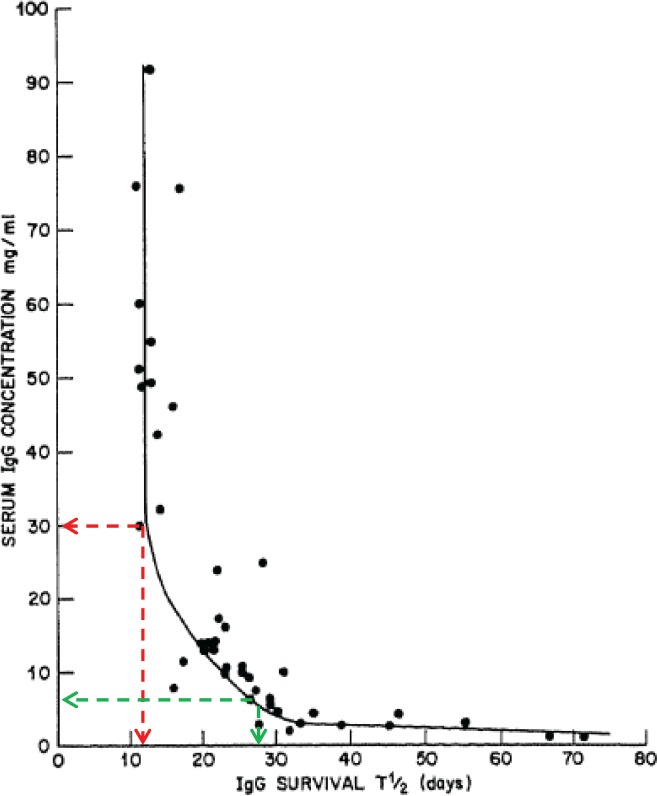
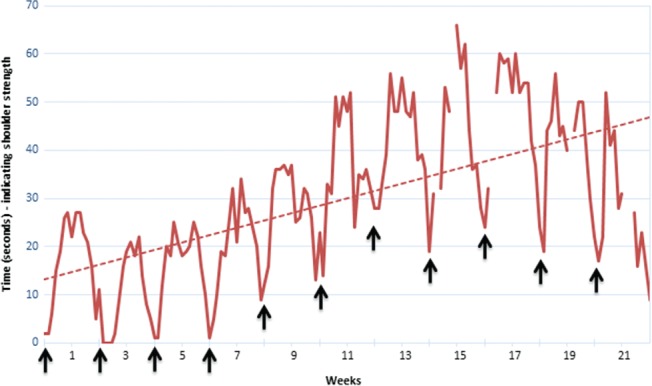
Despite the well-recognized importance of immunoglobulin therapy individualization during the treatment of chronic inflammatory demyelinating polyneuropathy (CIDP), the pathway to best achieve optimization is unknown. There are many pharmacokinetic and immunobiologic variables that can potentially influence the appropriateness of any individual therapy. Although identification of specific autoantibodies and their targets has only been accomplished in a minority of patients with CIDP, already the diagnostic and treatment implications of specific autoantibody detection are being realized. Individual variability in IgG pharmacokinetic properties including IgG catabolic rates and distribution, as well as the IgG level necessary for disease control also require consideration during the optimization process. For optimization to be successful there must be a measure of treatment response that has a clinically meaningful interpretation. There are currently available well-defined and validated clinical assessment tools and outcome measures that are well suited for this purpose. While there remains much to learn on how best to manipulate immunopathology and immunoglobulin pharmacokinetics in the most favorable way, there currently exists an understanding of these principles to a degree sufficient to begin to develop rational and evidence-based treatment optimization strategies.
Keywords: autoimmune neuromuscular diseases; chronic inflammatory demyelinating polyneuropathy; immune-mediated neuropathies; intravenous immunoglobulin; pharmacokinetics.
© 2018 The Authors. Journal of the Peripheral Nervous System published by Wiley Periodicals, Inc. on behalf of Peripheral Nerve Society.
Figures
References
-
- Allen JA, Lewis RA (2015). CIDP diagnostic pitfalls and perception of treatment benefit. Neurology 85:498–504. - PubMed
-
- Allen JA, Ney J, Lewis RA (2018). Electrodiagnostic errors contribute to chronic inflammatory demyelinating polyneuropathy misdiagnosis. Muscle Nerve 57:542–549. - PubMed
-
- Attarian S, Verschueren A, Franques J, Salort‐Campana E, Jouve E, Pouget J (2011). Response to treatment in patients with Lewis‐Sumner syndrome. Muscle Nerve 44:179–184. - PubMed
-
- Berger M (2004). Subcutaneous immunoglobulin replacement in primary immunodeficiencies. Clin Immunol 112:1–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
