

Heterozygosity for the alpha-1-antitrypsin Z allele in cirrhosis is associated with more advanced disease
- PMID: 29573137
- PMCID: PMC6032913
- DOI: 10.1002/lt.25057
Heterozygosity for the alpha-1-antitrypsin Z allele in cirrhosis is associated with more advanced disease
Abstract
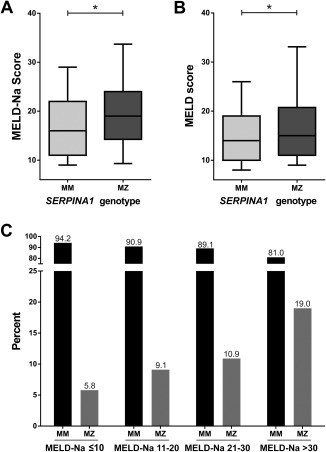
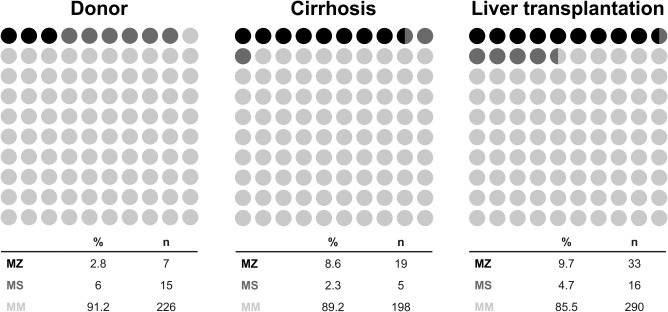
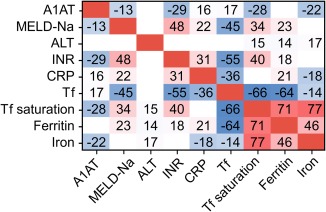
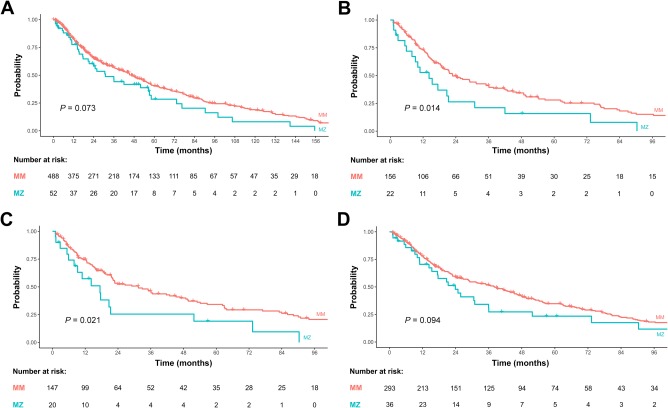
Alpha-1-antitrypsin deficiency (A1ATD) due to homozygosity for the Z allele (ZZ) is an established risk factor for cirrhosis, but the liver disease risk in heterozygous Z allele carriers (MZ) is controversial. The aim of the present study was to determine the prevalence of the MZ genotype among patients with cirrhosis and the associated risk of decompensation and liver transplantation/mortality. An unselected cohort of 561 patients with cirrhosis and 248 deceased liver donors were genotyped for the A1ATD risk alleles Z and S using a validated allelic discrimination assay. Clinical and biochemical parameters were assessed in 488 genotype MM and 52 MZ patients at baseline when cirrhosis was diagnosed and at the last contact, before liver transplantation or death, as study endpoints. MZ prevalence was 2.8% among liver donors, 5.8%, 9.1%, 10.9%, and 19.0% in patients with cirrhosis and Model for End-Stage Liver Disease-sodium (MELD-Na) ≤10, 11-20, 21-30, and >30, respectively. Among liver transplant recipients, MZ prevalence was 9.7%. MS prevalence was not different between donors, patients with cirrhosis, or transplant recipients. At the end of follow-up, MELD-Na scores were higher among heterozygous Z risk allele carriers (16 versus 19; P = 0.03). Decompensation of cirrhosis with ascites or encephalopathy was significantly more frequent in patients with MZ than in MM patients. In the subgroup with transferrin (Tf) saturation >50% or Tf <180 mg/dL, MZ patients had a significantly higher risk of liver transplantation or death than MM patients. In conclusion, the genotype MZ is a genetic risk factor for more advanced cirrhosis and decompensation. MZ patients with cirrhosis and hypotransferrinemia or increased Tf saturation are at higher risk of death and liver transplantation. Liver Transplantation 24 744-751 2018 AASLD.
© 2018 The Authors Liver Transplantation published by Wiley Periodicals, Inc. on behalf of American Association for the Study of Liver Diseases.
Figures

Comment in
-
Heterozygosity for the Alpha-1-Antitrypsin Z Allele in Cirrhosis Is Associated With More Advanced Disease.Liver Transpl. 2019 Feb;25(2):342-343. doi: 10.1002/lt.25393. Liver Transpl. 2019. PMID: 30525305 No abstract available.
-
Reply.Liver Transpl. 2019 Feb;25(2):344-345. doi: 10.1002/lt.25392. Liver Transpl. 2019. PMID: 30702813 No abstract available.
-
Heterozygosity for the Alpha-1-Antitrypsin Z Allele in Cirrhosis Is Associated With More Advanced Disease.Liver Transpl. 2019 Aug;25(8):1285-1286. doi: 10.1002/lt.25487. Epub 2019 Jun 25. Liver Transpl. 2019. PMID: 31077535 No abstract available.
-
Reply.Liver Transpl. 2019 Aug;25(8):1287-1288. doi: 10.1002/lt.25500. Epub 2019 Jun 25. Liver Transpl. 2019. PMID: 31120619 No abstract available.
References
-
- Greene CM, Marciniak SJ, Teckman J, Ferrarotti I, Brantly ML, Lomas DA, et al. α1‐antitrypsin deficiency. Nat Rev Dis Primers 2016;2:16051. - PubMed
-
- Chu AS, Chopra KB, Perlmutter DH. Is severe progressive liver disease caused by alpha‐1‐antitrypsin deficiency more common in children or adults? Liver Transpl 2016;22:886‐894. - PubMed
-
- Teckman JH, Rosenthal P, Abel R, Bass LM, Michail S, Murray KF, et al.; for Childhood Liver Disease Research Network (ChiLDReN) . Baseline analysis of a young alpha‐1‐antitrypsin deficiency liver disease cohort reveals frequent portal hypertension. J Pediatr Gastroenterol Nutr 2015;61:94‐101. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
