

Multiple drug intolerance syndrome and multiple drug allergy syndrome: Epidemiology and associations with anxiety and depression
- PMID: 29574787
- PMCID: PMC6157012
- DOI: 10.1111/all.13440
Multiple drug intolerance syndrome and multiple drug allergy syndrome: Epidemiology and associations with anxiety and depression
Abstract
Background: The epidemiology of multiple drug intolerance syndrome (MDIS) and multiple drug allergy syndrome (MDAS) is poorly characterized. We used electronic health record (EHR) data to describe prevalences of MDIS and MDAS and to examine associations with anxiety and depression.
Methods: Patients with ≥3 outpatient encounters at Partners HealthCare System from 2008 to 2015 were included. Patients with MDIS had intolerances to ≥3 drug classes, and patients with MDAS had hypersensitivities to ≥2 drug classes. Psychiatric conditions and comorbidities were defined from the EHR and used in multivariable logistic regression models to assess the relation between anxiety/depression and MDIS/MDAS.
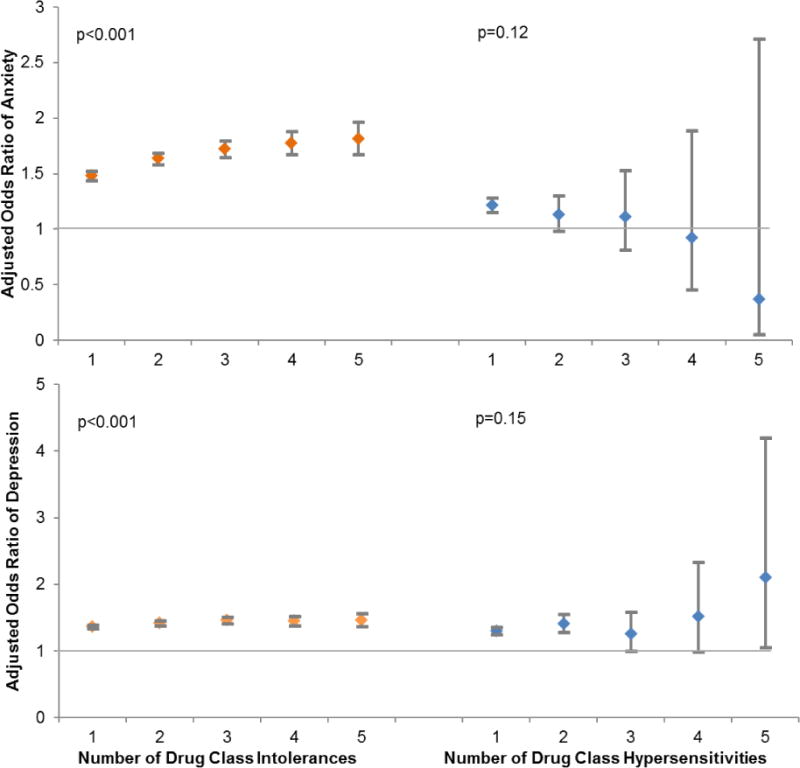
Results: Of 746 888 patients, 47 634 (6.4%) had MDIS and 8615 (1.2%) had MDAS; 3171 (0.4%) had both. Anxiety (adjusted odds ratio [aOR] 1.72 [1.65, 1.80]), depression (aOR 1.46 [1.41, 1.52]), and both anxiety and depression (aOR 1.97 [1.86, 2.08]) were associated with increased odds of MDIS. Depression was associated with increased odds of MDAS (aOR 1.41 [1.28, 1.56]), but there were no clear associations with anxiety (aOR 1.13 [0.99, 1.30]) nor both depression and anxiety (aOR 1.13 [0.92, 1.38]).
Conclusion: While 6% of patients had MDIS, only 1% had MDAS. MDIS was associated with both anxiety and depression; patients with both anxiety and depression had an almost twofold increased odds of MDIS. MDAS was associated with a 40% increased odds of depression, but there was no significant association with anxiety. Psychological assessments may be useful in the evaluation and treatment of patients with MDIS and MDAS; physiologic causes for MDAS warrant further investigation.
Keywords: anxiety; depression; healthcare utilization; hypersensitivity; immunologic.
© 2018 EAACI and John Wiley and Sons A/S. Published by John Wiley and Sons Ltd.
Conflict of interest statement
Figures
References
-
- Zhou L, Dhopeshwarkar N, Blumenthal KG, Goss F, Topaz M, Slight SP, et al. Drug allergies documented in electronic health records of a large healthcare system. Allergy. 2016;71:1305–13. - PubMed
-
- Macy E, Ho NJ. Multiple drug intolerance syndrome: Prevalence, clinical characteristics, and management. Ann Allergy Asthma Immunol. 2012;108:88–93. - PubMed
-
- Macy E. Multiple antibiotic allergy syndrome. Immunol Allergy Clin North Am. 2004;24:533–43. viii. - PubMed
-
- Lange L, Koningsbruggen SV, Rietschel E. Questionnaire-based survey of lifetime-prevalence and character of allergic drug reactions in German children. Pediatr Allergy Immunol. 2008;19:634–8. - PubMed
-
- Gomes E, Cardoso MF, Praca F, Gomes L, Marino E, Demoly P. Self-reported drug allergy in a general adult Portuguese population. Clin Exp Allergy. 2004;34:1597–601. - PubMed
Publication types
MeSH terms
Grants and funding
- K01 AI125631/AI/NIAID NIH HHS/United States
- K01AI125631/the National Institute of Allergy and Infectious Diseases (NIAID)/International
- the American Academy of Allergy, Asthma and Immunology (AAAAI) Foundation/International
- R01 HS022728/HS/AHRQ HHS/United States
- R01HS022728/Agency for Healthcare Research and Quality (AHRQ)/International
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
