

Acromegalic cardiomyopathy: Epidemiology, diagnosis, and management
- PMID: 29574794
- PMCID: PMC6489905
- DOI: 10.1002/clc.22867
Acromegalic cardiomyopathy: Epidemiology, diagnosis, and management
Abstract
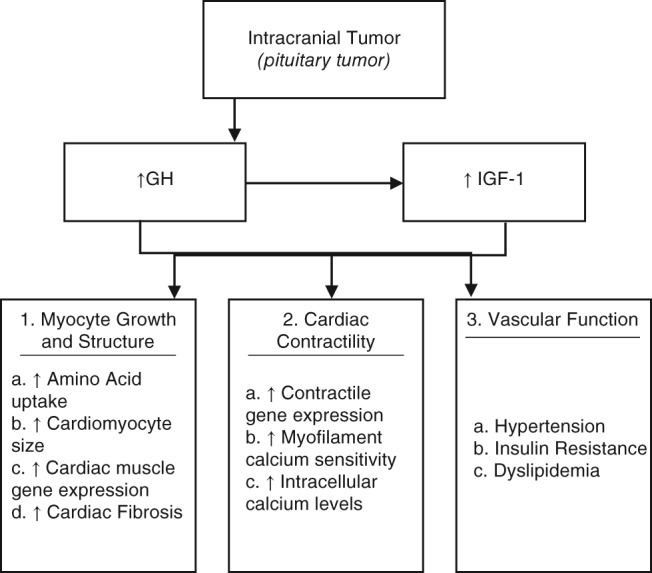
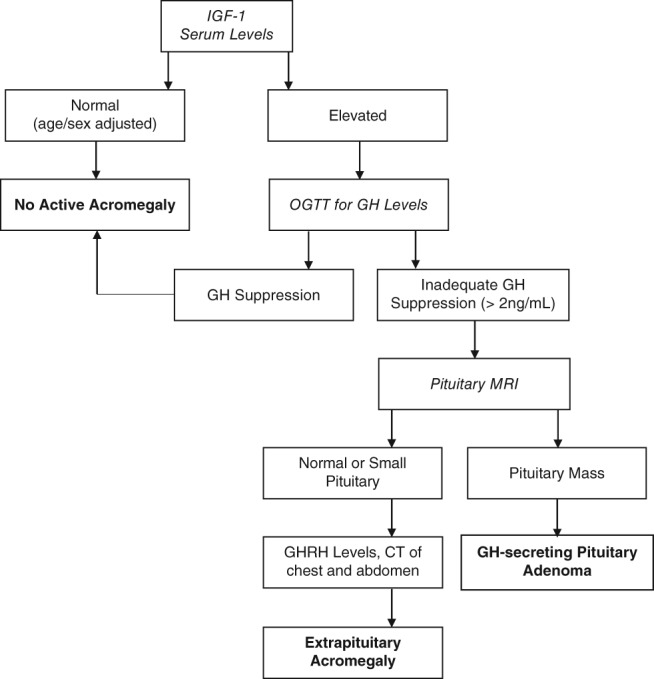
Acromegalic cardiomyopathy is the leading cause of morbidity and all-cause mortality in patients with acromegaly. Though acromegaly is a rare condition, the associated derangements are vast and severe. Stemming from an increase in circulating growth hormone (GH) and insulin-like growth factor-1 levels (IGF-1), acromegalic cardiomyopathy results in pathological changes in myocyte growth and structure, cardiac contractility, and vascular function. These molecular changes manifest commonly as biventricular hypertrophy, diastolic and systolic dysfunction, and valvular regurgitation. Early recognition of the condition is paramount, though the insidious progression of the disease commonly results in a late diagnosis. Biochemical testing, based on IGF-1 measurements, is the gold standard of diagnosis. Management should be centered on normalizing serum levels of both IGF-1 and GH. Transsphenoidal resection remains the most cost-effective and permanent treatment for acromegaly, though medical therapy possesses benefit for those who are not surgical candidates. Ultimately, achieving control of hormone levels results in a severe reduction in mortality rate, underscoring the importance of early recognition and treatment.
Keywords: Acromegalic Cardiomyopathy; Acromegaly; Clinical Manifestations; Diagnosis; Epidemiology; Prognosis.
© 2018 Wiley Periodicals, Inc.
Conflict of interest statement
The authors declare no potential conflicts of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
