

Healthcare-resource utilization associated with radiation to bone across eight European countries: Results from a retrospective study
- PMID: 29577024
- PMCID: PMC5865076
- DOI: 10.1016/j.jbo.2018.01.003
Healthcare-resource utilization associated with radiation to bone across eight European countries: Results from a retrospective study
Abstract
Background: Bone metastases and lytic lesions due to multiple myeloma are common in advanced cancer and can lead to debilitating complications (skeletal-related events [SREs]), including requirement for radiation to bone. Despite the high frequency of radiation to bone in patients with metastatic bone disease, our knowledge of associated healthcare resource utilization (HRU) is limited.
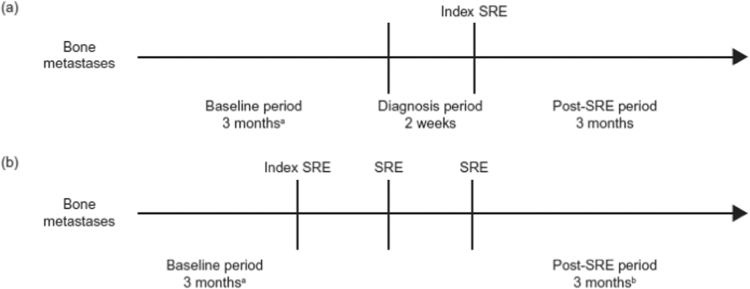
Methods: This retrospective study estimated HRU following radiation to bone in Austria, the Czech Republic, Finland, Greece, Poland, Portugal, Sweden and Switzerland. Eligible patients were ≥ 20 years old, had bone metastases secondary to breast, lung or prostate cancer, or bone lesions associated with multiple myeloma, and had received radiation to bone between 1 July 2004 and 1 July 2009. HRU data were extracted from hospital patient charts from 3.5 months before the index SRE (radiation to bone preceded by a SRE-free period of ≥ 6.5 months) until 3 months after the last SRE that the patient experienced during the study period.
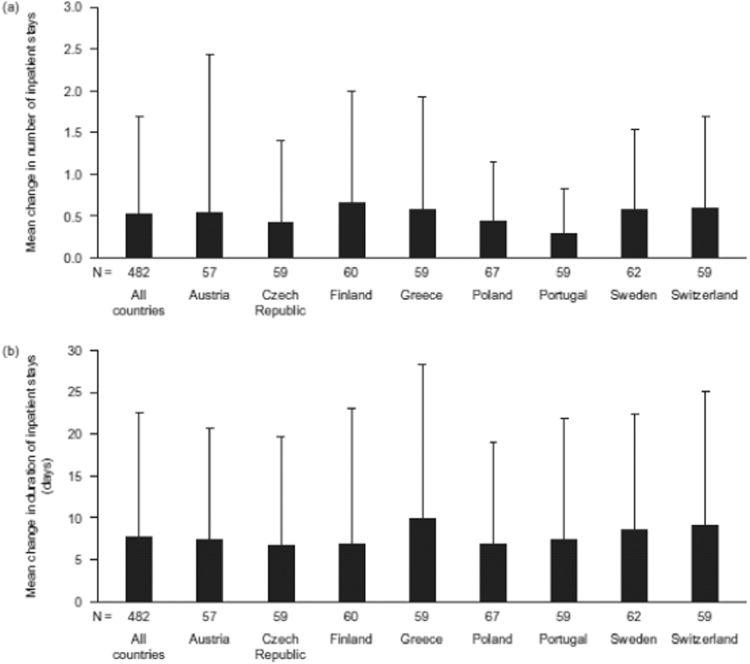
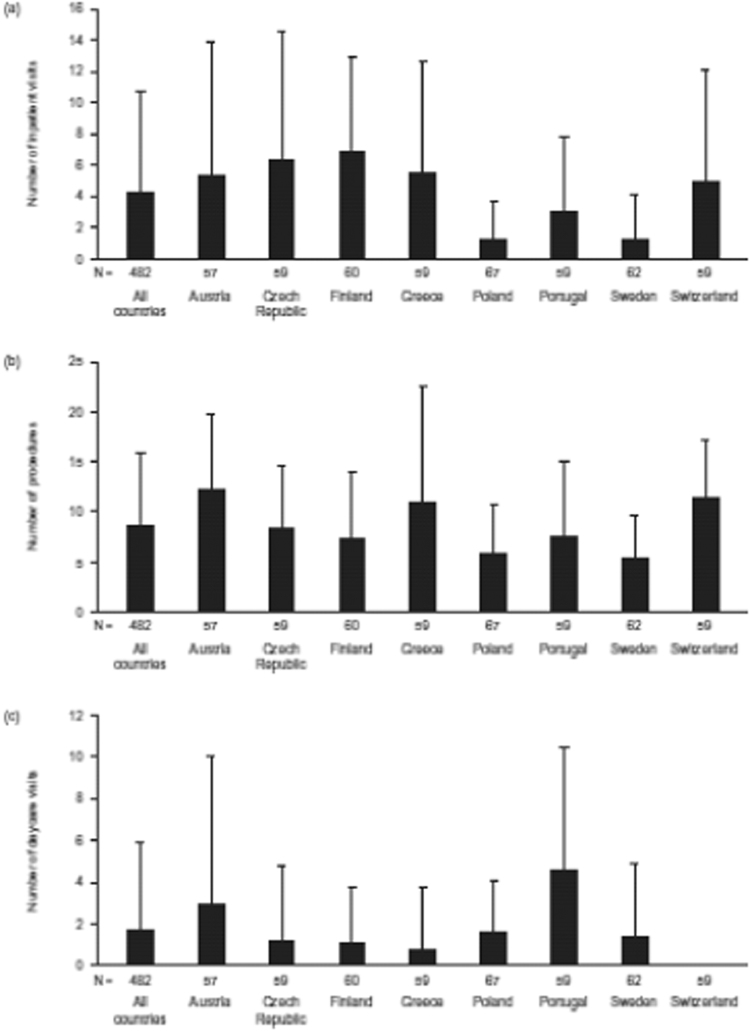
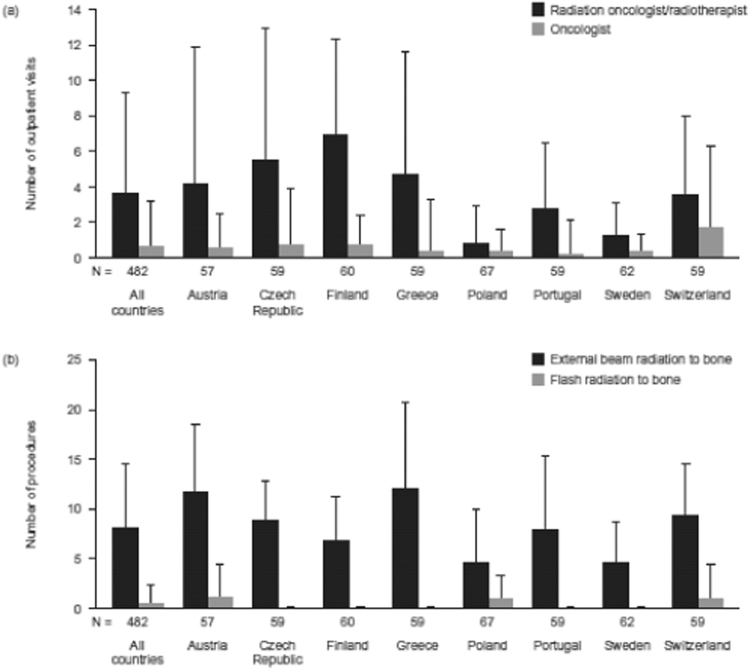
Results: In total, 482 patients were included. The number of inpatient stays increased from baseline by a mean of 0.52 (standard deviation [SD] 1.17) stays per radiation to bone event and the duration of stays increased by a mean of 7.8 (SD 14.8) days. Outpatient visits increased by a mean of 4.24 (SD 6.57) visits and procedures by a mean of 8.51 (SD 7.46) procedures.
Conclusion: HRU increased following radiation to bone across all countries studied. Agents that prevent severe pain and delay the need for radiation have the potential to reduce the burden imposed on healthcare resources and patients.
Keywords: Bone metastases; Bone pain; Health resource utilization; Radiation to bone; Skeletal-related event.
Figures
Similar articles
-
Health resource utilization associated with skeletal-related events: results from a retrospective European study.Eur J Health Econ. 2016 Jul;17(6):711-21. doi: 10.1007/s10198-015-0716-7. Epub 2015 Aug 8. Eur J Health Econ. 2016. PMID: 26253584 Free PMC article.
-
Pathologic fracture and healthcare resource utilisation: A retrospective study in eight European countries.J Bone Oncol. 2016 Sep 12;5(4):185-193. doi: 10.1016/j.jbo.2016.07.003. eCollection 2016 Nov. J Bone Oncol. 2016. PMID: 28008381 Free PMC article.
-
Cost of skeletal complications from bone metastases in six European countries.J Med Econ. 2016 Jun;19(6):611-8. doi: 10.3111/13696998.2016.1150852. Epub 2016 Feb 23. J Med Econ. 2016. PMID: 26849381
-
Pharmacoeconomics of bisphosphonates for skeletal-related event prevention in metastatic non-breast solid tumours.Pharmacoeconomics. 2012 May;30(5):373-86. doi: 10.2165/11631390-000000000-00000. Pharmacoeconomics. 2012. PMID: 22500986 Review.
-
Zoledronic acid: a review of its use in the management of bone metastases and hypercalcaemia of malignancy.Drugs. 2003;63(4):417-37. doi: 10.2165/00003495-200363040-00009. Drugs. 2003. PMID: 12558465 Review.
References
-
- Coleman R.E. Metastatic bone disease: clinical features, pathophysiology and treatment strategies. Cancer Treat. Rev. 2001;27(3):165–176. - PubMed
-
- von Moos R., Body J.J., Egerdie B., Stopeck A., Brown J.E., Damyanov D., Fallowfield L.J., Marx G., Cleeland C.S., Patrick D.L., Palazzo F.G., Qian Y., Braun A., Chung K. Pain and health-related quality of life in patients with advanced solid tumours and bone metastases: integrated results from three randomized, double-blind studies of denosumab and zoledronic acid. Support Care Cancer. 2013;21(12):3497–3507. - PubMed
-
- WHO, WHO’s Cancer Pain Ladder for Adults. 〈http://www.who.int/cancer/palliative/painladder/en〉. (accessed 26 January 2017).
-
- Ripamonti C.I., Santini D., Maranzano E., Berti M., Roila F., Group E.G.W. Management of cancer pain: ESMO Clinical Practice Guidelines. Ann. Oncol. 2012;23(Suppl. 7) (vii139–54) - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
