

Chylous Ascites: A Review of Pathogenesis, Diagnosis and Treatment
- PMID: 29577037
- PMCID: PMC5863006
- DOI: 10.14218/JCTH.2017.00035
Chylous Ascites: A Review of Pathogenesis, Diagnosis and Treatment
Abstract
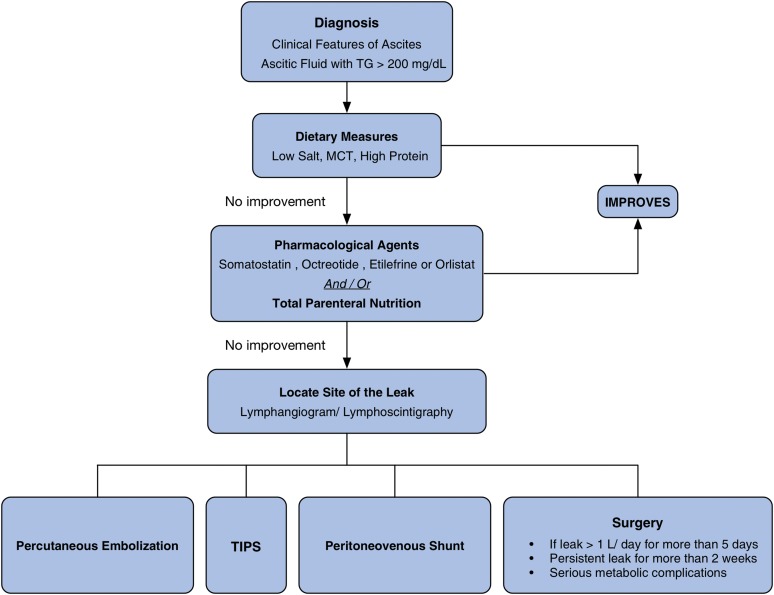
Chylous ascites (CA) is a rare form of ascites that results from the leakage of lipid-rich lymph into the peritoneal cavity. This usually occurs due to trauma and rupture of the lymphatics or increased peritoneal lymphatic pressure secondary to obstruction. The underlying etiologies for CA have been classified as traumatic, congenital, infectious, neoplastic, postoperative, cirrhotic or cardiogenic. Since malignancy and cirrhosis account for about two-thirds of all the cases of CA in Western countries, in this article we have attempted to reclassify CA based on portal and non-portal etiologies. The diagnosis of CA is based on the distinct characteristic of the ascitic fluid which includes a milky appearance and a triglyceride level of >200 mg/dL. The management consists of identifying and treating the underlying disease process, dietary modification, and diuretics. Some studies have also supported the use of agents such as orlistat, somatostatin, octreotide and etilefrine. Paracentesis and surgical interventions in the form of transjugular intrahepatic portosystemic shunt (commonly known as TIPS), peritoneal shunt, angiography with embolization of a leaking vessel, and laparotomy remain as treatment options for cases refractory to medical management.
Keywords: Ascitic fluid; Chylous ascites; Cirrhosis; Lymphatic system; Portal hypertension.
Conflict of interest statement
The authors have no conflict of interests related to this publication.
Figures




References
-
- Browse NL, Wilson NM, Russo F, al-Hassan H, Allen DR. Aetiology and treatment of chylous ascites. Br J Surg. 1992;79:1145–1150. doi: 10.1002/bjs.1800791110. - DOI - PubMed
-
- Aalami OO, Allen DB, Organ CH., Jr Chylous ascites: a collective review. Surgery. 2000;128:761–778. doi: 10.1067/msy.2000.109502. - DOI - PubMed
-
- Cárdenas A, Chopra S. Chylous ascites. Am J Gastroenterol. 2002;97:1896–1900. doi: 10.1111/j.1572-0241.2002.05911.x. - DOI - PubMed
-
- Khoury T, Schneider R. Chylous ascites: a rare adverse effect of methimazole treatment for grave’s disease-a case report and review of the literature. Case Rep Endocrinol. 2015;2015:649303. doi: 10.1155/2015/649303. - DOI - PMC - PubMed
-
- Capristo E, Spuntarelli V, Treglia G, Arena V, Giordano A, Mingrone G. A case report of chylous ascites after gastric bypass for morbid obesity. Int J Surg Case Rep. 2016;29:133–136. doi: 10.1016/j.ijscr.2016.10.077. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources