

Training contraceptive providers to offer intrauterine devices and implants in contraceptive care: a cluster randomized trial
- PMID: 29577915
- PMCID: PMC5970088
- DOI: 10.1016/j.ajog.2018.03.016
Training contraceptive providers to offer intrauterine devices and implants in contraceptive care: a cluster randomized trial
Abstract
Background: US unintended pregnancy rates remain high, and contraceptive providers are not universally trained to offer intrauterine devices and implants to women who wish to use these methods.
Objective: We sought to measure the impact of a provider training intervention on integration of intrauterine devices and implants into contraceptive care.
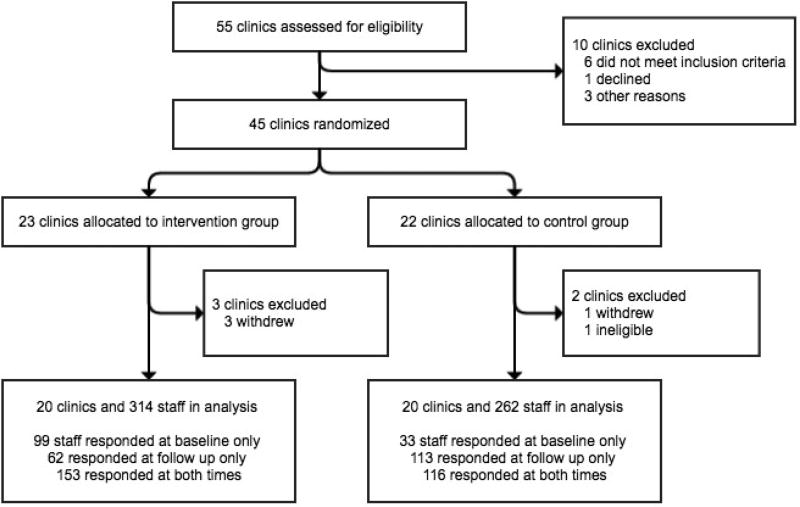
Study design: We measured the impact of a continuing medical education-accredited provider training intervention on provider attitudes, knowledge, and practices in a cluster randomized trial in 40 US health centers from 2011 through 2013. Twenty clinics were randomly assigned to the intervention arm; 20 offered routine care. Clinic staff participated in baseline and 1-year surveys assessing intrauterine device and implant knowledge, attitudes, and practices. We used a difference-in-differences approach to compare changes that occurred in the intervention sites to changes in the control sites 1 year later. Prespecified outcome measures included: knowledge of patient eligibility for intrauterine devices and implants; attitudes about method safety; and counseling practices. We used multivariable regression with generalized estimating equations to account for clustering by clinic to examine intervention effects on provider outcomes 1 year later.
Results: Overall, we surveyed 576 clinic staff (314 intervention, 262 control) at baseline and/or 1-year follow-up. The change in proportion of providers who believed that the intrauterine device was safe was greater in intervention (60% at baseline to 76% at follow-up) than control sites (66% at both times) (adjusted odds ratio, 2.48; 95% confidence interval, 1.13-5.4). Likewise, for the implant, the proportion increased from 57-77% in intervention, compared to 61-65% in control sites (adjusted odds ratio, 2.57; 95% confidence interval, 1.44-4.59). The proportion of providers who believed they were experienced to counsel on intrauterine devices also increased in intervention (53-67%) and remained the same in control sites (60%) (adjusted odds ratio, 1.89; 95% confidence interval, 1.04-3.44), and for the implant increased more in intervention (41-62%) compared to control sites (48-50%) (adjusted odds ratio, 2.30; 95% confidence interval, 1.28-4.12). Knowledge scores of patient eligibility for intrauterine devices increased at intervention sites (from 0.77-0.86) 6% more over time compared to control sites (from 0.78-0.80) (adjusted coefficient, 0.058; 95% confidence interval, 0.003-0.113). Knowledge scores of eligibility for intrauterine device and implant use with common medical conditions increased 15% more in intervention (0.65-0.79) compared to control sites (0.67-0.66) (adjusted coefficient, 0.15; 95% confidence interval, 0.09-0.21). Routine discussion of intrauterine devices and implants by providers in intervention sites increased significantly, 71-87%, compared to in control sites, 76-82% (adjusted odds ratio, 1.97; 95% confidence interval, 1.02-3.80).
Conclusion: Professional guidelines encourage intrauterine device and implant competency for all contraceptive care providers. Integrating these methods into routine care is important for access. This replicable training intervention translating evidence into care had a sustained impact on provider attitudes, knowledge, and counseling practices, demonstrating significant changes in clinical care a full year after the training intervention.
Keywords: continuing education; contraception; contraceptive implant; intrauterine device; provider training intervention.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Obstetrics-gynecology resident long-acting reversible contraception training: the role of resident and program characteristics.Am J Obstet Gynecol. 2020 Apr;222(4S):S923.e1-S923.e8. doi: 10.1016/j.ajog.2019.12.007. Epub 2019 Dec 19. Am J Obstet Gynecol. 2020. PMID: 31866517
-
Funding policies and postabortion long-acting reversible contraception: results from a cluster randomized trial.Am J Obstet Gynecol. 2016 Jun;214(6):716.e1-8. doi: 10.1016/j.ajog.2015.12.009. Epub 2015 Dec 12. Am J Obstet Gynecol. 2016. PMID: 26692178 Free PMC article. Clinical Trial.
-
Familiarity and acceptability of long-acting reversible contraception and contraceptive choice.Am J Obstet Gynecol. 2020 Apr;222(4S):S884.e1-S884.e9. doi: 10.1016/j.ajog.2019.11.1266. Epub 2019 Dec 12. Am J Obstet Gynecol. 2020. PMID: 31838124 Free PMC article.
-
Intrauterine contraceptive device training and outcomes for healthcare providers in developed countries: A systematic review.PLoS One. 2019 Jul 15;14(7):e0219746. doi: 10.1371/journal.pone.0219746. eCollection 2019. PLoS One. 2019. PMID: 31306443 Free PMC article.
-
A Decision Aid to Help Women Choose and Use a Method of Birth Control [Internet].Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2019 Oct. Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2019 Oct. PMID: 36888734 Free Books & Documents. Review.
Cited by
-
Exploring adolescent-facing US clinicians' perceptions of their contraceptive counseling and use of shared decision-making: A qualitative study.Perspect Sex Reprod Health. 2024 Dec;56(4):337-346. doi: 10.1111/psrh.12283. Epub 2024 Aug 22. Perspect Sex Reprod Health. 2024. PMID: 39175306
-
Barriers and facilitators to contraception provision among rural healthcare providers.Contracept Reprod Med. 2025 Mar 10;10(1):17. doi: 10.1186/s40834-025-00350-x. Contracept Reprod Med. 2025. PMID: 40059209 Free PMC article.
-
Is there a difference in the clinical profile and outcome of women using levonorgestrel IUD for abnormal uterine bleeding and those using it for contraception?: A comparative cross-sectional study.Turk J Obstet Gynecol. 2024 Mar 4;21(1):7-14. doi: 10.4274/tjod.galenos.2024.51460. Turk J Obstet Gynecol. 2024. PMID: 38440962 Free PMC article.
-
Identification of Clinician Training Techniques as an Implementation Strategy to Improve Maternal Health: A Scoping Review.Int J Environ Res Public Health. 2023 May 30;20(11):6003. doi: 10.3390/ijerph20116003. Int J Environ Res Public Health. 2023. PMID: 37297607 Free PMC article.
-
Providers' approaches to contraceptive provision in Cape Town.Front Glob Womens Health. 2022 Sep 14;3:917881. doi: 10.3389/fgwh.2022.917881. eCollection 2022. Front Glob Womens Health. 2022. PMID: 36188423 Free PMC article.
References
-
- Donnelly KZ, Foster TC, Thompson R. What matters most? The content and concordance of patients' and providers' information priorities for contraceptive decision making. Contraception. 2014;90:280–7. - PubMed
-
- Stanwood NL, Garrett JM, Konrad TR. Obstetrician-gynecologists and the intrauterine device: a survey of attitudes and practice. Obstet Gynecol. 2002;99:275–80. - PubMed
-
- Harper CC, Blum M, de Bocanegra HT, et al. Challenges in translating evidence to practice: The provision of intrauterine contraception. Obstet Gynecol. 2008;111:1359–69. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
